Chapter: Forensic Medicine: Firearm injuries
Firearm injuries
Firearm injuries
Introduction
Although firearms also include arms that can
fire plastic and rubber bullets, as well as industrial nailguns, it is
especially pistols, revolvers and rifles which are important. This group of
firearms is divided into handarms and shoulderarms, and also according to
whether the barrel is rifled or not. Rifled firearms have spiral grooves on the
inner surface of the barrel which gives the spinning movement to the projectile
as it travels down the barrel. This rotational movement or spin stabilises the
projectile in flight. Handarms, for example revolvers and pistols, as well as
shoulderarms such as hunting rifles, and automatic and semi-automatic machine
guns, all have these grooves. Smooth-bore firearms (eg shotguns) do not have
grooves.
When the percussion pin activated by the trigger
strikes the percussion cap, the spark generated ignites the propellant powder
in the bullet casing. This powder has chemical and physical characteristics
peculiar to the type of ammunition. The gases which develop during the explosion
have a potential volume many times greater than that of the powder, generally
in excess of 500 times under atmospheric pressure. It is this gas pressure
which drives the projectile along the barrel. While passing along the barrel
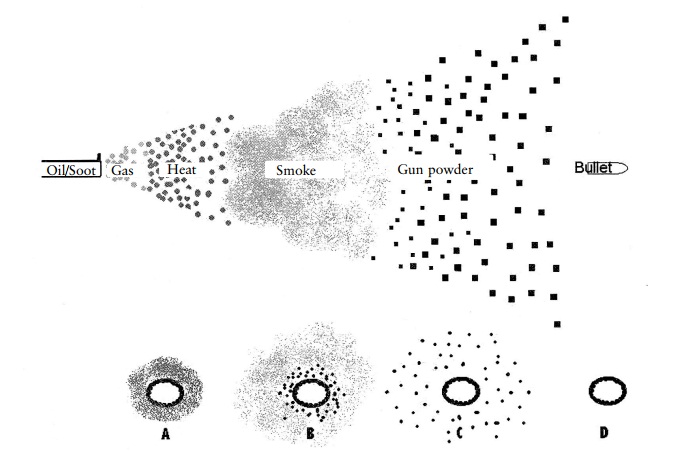
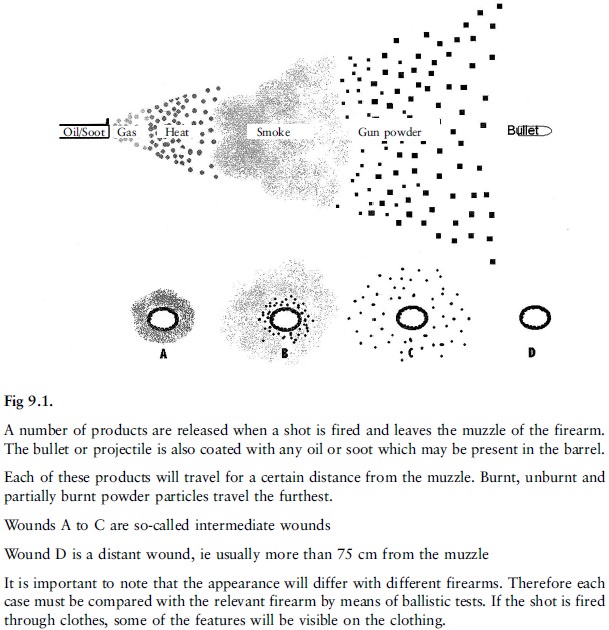
the projectile is soiled by oil and gas in the barrel. When it leaves the
muzzle there is also a flash and a gas emission, which includes carbon
monoxide, as well as hot and partially unignited powder particles, all of which
impart to the recipient surface characteristics which assist in determining the
firing range for that particular weapon and its ammunition.
Although the medical practitioner is not a
ballistics expert the observations made in the case of firearm injuries can be
of considerable assistance in establishing the range as well as the direction
of fire, the type and calibre of weapon and the nature of the wound, for
example whether it points at suicide, homicide or an accident. Then, and
equally relevant, there is the establishment of (in the case of fatal injury)
the manner of death as well as the period of survival and the extent of
immobilisation of the victim and restriction of volitional acts on account of
the injury.
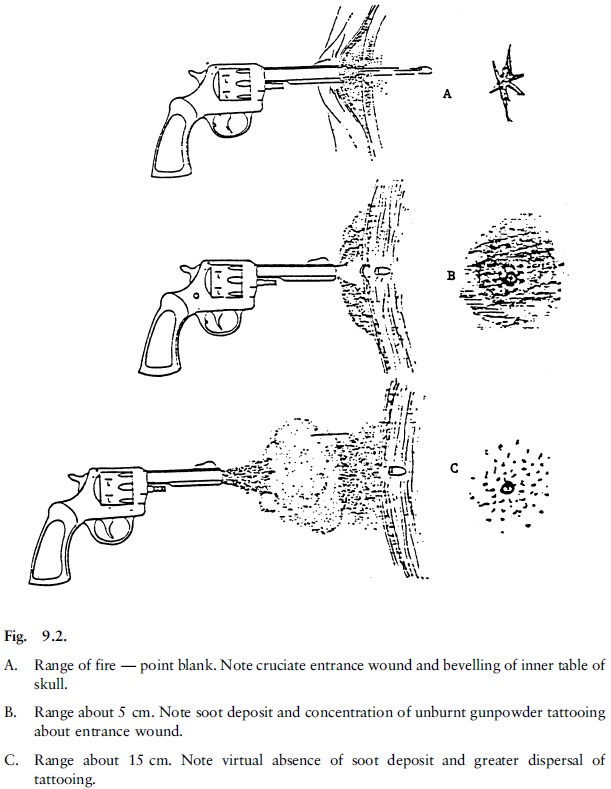
In order to measure up to the expectations of
the court in this regard, close attention must be paid to the size and shape of
the entrance and exit wound(s). Careful inspection of the skin around the
entrance wound, noting the presence, size and shape of any abrasion collar,
smoke blackening, tattooing and singeing of hair, is an essential element of
the medical investigation. Evidence should also be sought of any vital
reaction, such as erythema (a reddening of the skin) in the vicinity of
hot-powder tattooing and carboxyhaemoglobin in surrounding tissues (carbon
monoxide is one of the gases emitted by the explosion in the chamber of the
firearm).
An X-ray examination of the body (both at the
clinical examination and the autopsy) can be of considerable assistance in
retrieving projectiles for ballistic examination, particularly in the case of
multiple entrance wounds.
In siting both entrance and exit wounds it is
helpful if measurements are expressed as the perpendicular height above the
base of the heel line. Entrance and exit wounds must preferably be indicated on
a diagram. This can assist (when evidence is given) to relate the findings to
circumstantial evidence. It must be remembered that the direction of the wound
track, with the body in the anatomical position during the post-mortem
examination, is not necessarily representative of the position of the body when
it was hit by the projectile. For instance, if the individual was slightly bent
over while running away, and then hit by a projectile fired at a horizontal
level, the entrance wound in the back may be lower than the exit wound at the front
if the body is in the anatomical position.
Caution should be exercised when expressing an
opinion on the pre-impact direction of the projectile flight path based solely
on the wound in the tissues after impact, as there can be considerable
deflection, not only through the bony structures, but also through the soft
tissues.
During clinical examination and autopsy other
evidence should be sought, such as powder marks on the hands of the victim and
assailant and other evidence of a struggle by either party. Clothing can absorb
much of the explosion residue and modify the shape of the entrance wound.
Therefore it should always form an integral part of the examination. Serious
omissions in the accumulation of medical evidence may result where no attempt
is made to anticipate the needs and priorities of the subsequent inquiry. This
is what happened initially at the autopsy of President Kennedy after his
assassination. (See Where Death Delights by Milton Helpern.)
Multiple firearm wounds do not necessarily rule
out suicide. In one case the deceased had three separate revolver wounds in the
chest and all three bullets had penetrated the ventricles of the heart. A
suicide note was found, the revolver was shown ballistically to have fired the
shots, and swabs taken from the deceased's right hand contained the specific
powder residue.
The percussion effect set up in the tissue by
shock waves during the projectile's flight is well exemplified in the following
case. A fugitive who was running away from the scene of a burglary, was fired
on at a range of about 40 metres while his trunk was flexed forward in a
position customarily adopted by escapees to reduce the target site. Despite
being hit by a shot, he continued to run for another 100 metres, before
collapsing. He died half an hour later. At the autopsy an entrance wound was
indentified above the left iliac crest, on the lateral side of the body. The
bullet had tracked upward in the subcutaneous tissues to enter the chest cavity
between the eighth and ninth ribs, and had then passed across the dome of the
diaphragm, below the parietal pleura, along the outer aspect of the pericardial
sac to come to rest in the apex of the left lung.
Neither the abdominal cavity nor the pericardial
sac had been penetrated by the projectile, yet the former contained 100 ml of
free blood and the pericardial sac 350 ml of blood, resulting from a 2 cm
percussion rupture of the liver, and 3 cm rupture of the left ventricle of the
heart .
Related Topics