Chapter: Forensic Medicine: Firearm injuries
Cutaneous (skin) entrance wounds caused by rifled firearms
Cutaneous (skin) entrance wounds caused by rifled
firearms
Introduction
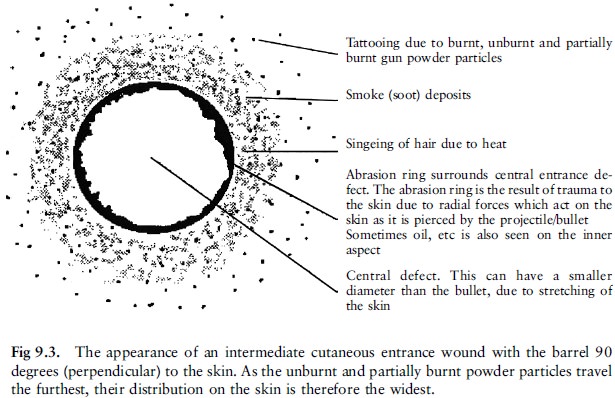
Entrance wounds are usually round or ovoid
(oval) with an abrasion ring where the bullet abraded the skin during entrance.
This abrasion ring is caused by the force exerted by the projectile at entry,
when the outermost layers of the epidermis are stripped away. It is not caused
by the rotational movement of the projectile, as it is sometimes described in
the literature, but by the tangential force exerted on the skin. Similar
abrasions are sometimes seen surrounding the exit wound when the skin is
pressed against a hard object, for instance a belt buckle. After the bullet
perforated the skin the elasticity of the cutaneous tissue restores the skin's
previous elasticity and the skin defect contracts.
When bullets strike skin at a 908 angle (ie
perpendicular to the skin surface) they produce round entrance wounds with a
more or less symmetrical collar or abrasion ring. Oval or elliptical entrance
wounds with asymmetrical abrasion rings occur when bullets strike the skin at
acute angles. The wider area of abrasion is then located on the side of the
entrance wound closest to the gun.
Entrance wound shape (ie round, oval,
star-shaped or cross-shaped) and size must be described precisely. Cutaneous
injury and its associated features, such as soiling and rim abrasion ring,
should be accurately measured and the dimensions recorded. A circular wound
requires only the diameter measure-ment, whereas an elliptical wound is
measured across its widest and narrowest diameters and variations in width of
the marginal abrasion are recorded. Peripheral fouling or stippling due to
unburnt powder residues should be specifically noted.
Concealed and unusual entrance wounds
Entrance wounds occasionally occur in unusual
sites or are not easily seen. If the body is covered in blood, clots may
obscure the injury. Similarly, scalp and pubic wounds are not easily seen, and
in these cases shaving the hair before autopsy will reveal the injury. The
possibility of wounds in concealed or unusual sites should always be borne in
mind. Such sites comprise the external auditory meatus (opening), nostrils,
umbilicus (navel), axillae (armpits), perineum (pelvic floor), vagina and
rectum. Oral wounds are sometimes difficult to see as a bullet may have entered
the open mouth, and after rigor mortis set in the mouth could not be opened.
Injuries which do not look like gunshot wounds
can be difficult to interpret. This occurs for example when the missile passes
through glass or if the bullet strikes the body after it has ricocheted. If the
bullet then glances off the body without penetrating, only an abrasion or
laceration may be produced.
A round penetrating defect similar to a bullet
entrance wound can also be produced by an instrument such as a screwdriver, but
in this case no missile will be found at the end of the track. Similar wounds
can be produced if the victim was beaten with a nail-studded plank.
Classification of cutaneous gunshot entrance wounds
The definitive factor determining the appearance
of a cutaneous entrance wound is the muzzle-to-skin distance, which accounts
for the simple classification of entrance wounds as ``contact'',
``intermediate'' and ``distant''. However, estimates of the firing range cannot
be made with accuracy unless the exact type of firearm is known, and even then
only by ballistic experts, preferably after test shots were fired at varying
distances under controlled conditions.
Contact wounds
The margins of the skin perforation are charred
by the flame coming from the muzzle, and the abraded border is usually soiled
with powder residue which can also be clearly visible in the subcutaneous and
deeper tissues. The surrounding abrasion ring is of uniform width, and around
this there can be an additional abrasion ring from the gun barrel and gun
sight. These muzzle imprints result from expansion of the subcutaneous tissue
when gas is blown into the tissue, elevating the skin surface and pressing it
tightly against the muzzle. The subcutaneous tissues in and immediately
adjacent to the bullet track may have a cherry red colour due to localised
carboxyhaemoglobin formation from carbon monoxide in the muzzle gases. If the
muzzle is at an angle with the skin, the distribution is more elliptical.
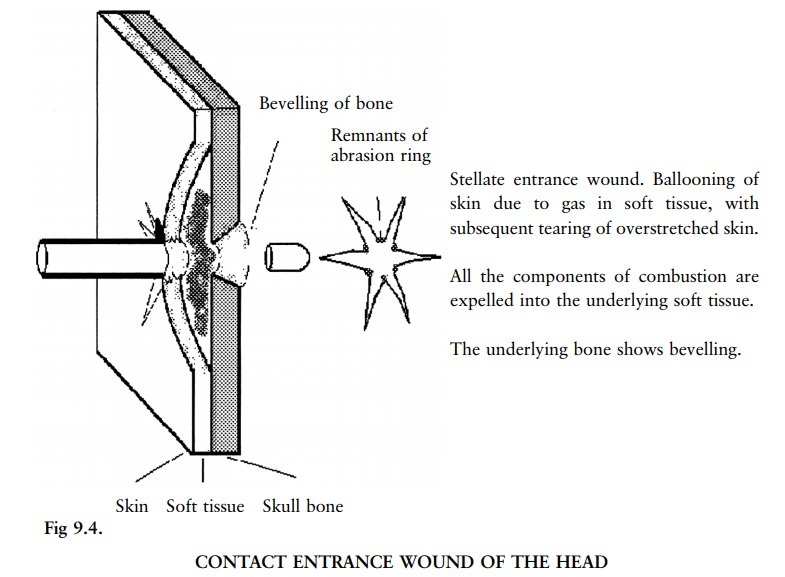
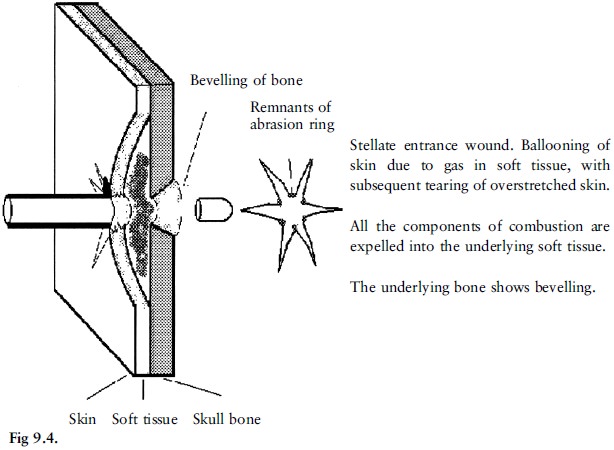
Contact-range entrance wounds in the scalp look
slightly different because stellate (star-shaped) lacerations radiate from the
central defect (fig 9.4). This is due to expansion of the explosion gases
between scalp and skull and within the cranial cavity. Explosion skull fractures
may result, producing bone fragments which can act as secondary missiles.
Intermediate or medium distance entrance wounds
Entrance gunshot wounds are classified as
intermediary when muzzle-to-target distances are such that the target surface
is still within range of the muzzle blast although target and muzzle are not in
contact. Maximum muzzle-to-target distances at which flame and muzzle blast
create dermal damage and soiling vary according to the type of gun and
ammunition. Handguns and ammunition encountered in civilian homicides do not
ordinarily deposit powder on the target at ranges greater than 50 to 75 cm.
Close-range entrance wounds in unclothed areas may be surrounded by a radial
arrangement of soot and be singed by flame. If the wound is in a hairy area,
hair may be singed and examination with a hand lens may reveal clubbing of the
hair ends due to melting of the keratin.
Distant wounds
A distant wound may show a surrounding faint
zone of ecchymotic discoloration due to subcutaneous bleeding. Only the defect
where the bullet entered the skin, with a surrounding abrasion ring, is
evident.
Related Topics