Chapter: Basic Radiology : Gastrointestinal Tract
Exercise: Small-Bowel Obstruction
EXERCISE 10-4.
SMALL-BOWEL OBSTRUCTION
10-13. What is the most likely cause of the lucent band
(in-terconnected arrows) involving the terminal ileum (TI) and causing
small-bowel obstruction (arrow; C, cecum) in Case 10-13 (Figure 10-38)?

A.
Ileocolic intussusception
B.
Obstructing adhesions
C.
Meckel diverticulum
D.
Small-bowel volvulus
E.
Polypoid malignancy
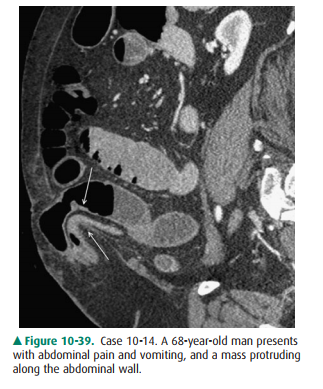
10-14. What is the most likely cause of the transition in
small-bowel caliber (arrows), which is causing ob-struction on this sagittal
reformatted CT scan in Case 10-14 (Figure 10-39)?
A.
Meckel diverticulum
B.
Small-bowel volvulus
C.
Adhesions with obstruction
D.
Polypoid small-bowel tumor
E.
Anterior abdominal wall hernia
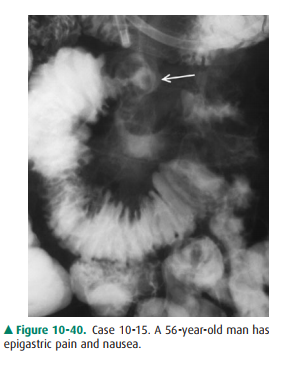
10-15. What is the least likely cause of the angulated focal
narrowing (arrow) seen on the enteroclysis examina-tion in Case 10-15 (Figure
10-40)?
A.
Carcinoid tumor
B.
Metastatic mass
C.
Small-bowel lymphoma
D.
Intussusception due to mass
E.
Small-bowel adenocarcinoma
10-16. What is the most likely cause of the multiple areas of
angulation and narrowing (arrows) causing small-bowel obstruction in Case 10-16
(Figure 10-41)?

A.
Peritoneal adhesions
B.
Small-bowel adenocarcinoma
C.
Metastatic disease
D.
Radiation enteritis
E.
Small-bowel intussusceptions
Radiologic Findings
10-13. The lucent band is due to adhesions causing a
distalsmall-bowel obstruction (B is the correct answer to Question 10-13).
10-14. A small-bowel loop is contained within an external
anterior abdominal wall hernia with narrowing of the lower small-bowel loop (E
is the correct answer to Question 10-14).
10-15. The irregular, angulated mass narrowing is likely due to
a small-bowel malignancy; a carcinoid tumor was found at surgery. A polypoid
mass with intussuscep-tion would appear as a focal dilatation of the bowel (D
is the correct answer to Question 10-15).
10-16. Multiple sites of narrowing and angulation (arrows) are
causing small-bowel obstruction; in a patient with a known malignancy,
peritoneal metastasis with serosal bowel involvement is the most likely cause
(C is the correct answer to Question 10-16).
Discussion
The most common causes of
small-bowel obstruction are ad-hesions, hernias, and primary or secondary
neoplasms of the small intestine. Although barium examinations of the small
bowel have been used traditionally to evaluate small-bowel obstruction, more modern
imaging using a variety of CT and MR techniques (as discussed previously) is
now used more often, particularly in the presence of high-grade bowel
ob-struction.
Peritoneal adhesions are most
often the cause of small-bowel obstruction in adults. Previous abdominal
surgery is the usual explanation for development of peritoneal adhe-sions.
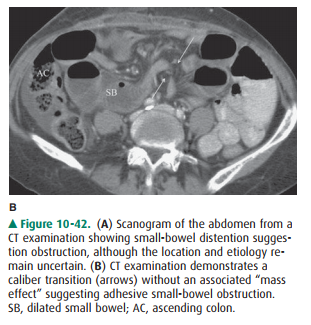
Focal small-bowel obstruction is diagnosed on con-trast examination and also
with cross-sectional imaging (ie, CT or MR) by demonstrating an area of caliber
transition from dilated to normal-caliber bowel. If angulated loops are seen at
a caliber transition in the absence of a mass effect, ad-hesions are the likely
cause of obstruction; these criteria are useful whether traditional contrast
examination or CT imag-ing is being used for evaluating patients with suspected
small-bowel obstruction (Figure 10-42).

Abdominal hernias are now
considered the second most common cause of small-bowel obstruction, and their
preva-lence and location will vary depending on the age and sex of the patient.
External hernias are the most common types, with the inguinal canal
predominating in the male popula-tion; however, hernias may occur in other
areas of the ab-domen, such as in the umbilical and paraumbilical regions.
Hernias can also be seen more laterally (eg, Spigelian type at the lateral
margin of the rectus muscle) and may be associ-ated with incisional scars from
previous abdominal surgery. CT examination of the abdomen with the ability to
reformat in a variety of planes (ie, coronal and sagittal) is an ideal im-aging
modality for evaluation of abdominal hernias. Internalhernias are much less
common, but may also be a cause of bowel obstruction.
Small-bowel malignancies were
discussed briefly in the previous exercise. Adenocarcinoma of the small bowel
oc-curs most often in the duodenum and jejunum and is muchless common in the
ileum. The morphologic appearance of adenocarcinomas of the small intestine
consists of poly-poid, ulcerative, stenosing, and infiltrative forms, which are
similar to their counterparts in the stomach and colon. Pri-mary lymphomas of
the small bowel are a heterogeneous group of tumors, and controversy persists
regarding defini-tion of primary and secondary forms of this neoplasm.
Lymphomas may involve any level of the small intestine but are most common in
the ileum; the gross pathologic pat-terns include nodular or polypoid masses,
constricting le-sions that resemble carcinoma, or a more diffusely nodular or
infiltrative process.

Carcinoid tumor and malignant GIST
are the other two primary malignancies seen in the small bowel. GIST usu-ally
occurs as a single lesion and is most often found in the jejunum and ileum.
Pathologically, this tumor typically presents as a polypoid mass with an
intraluminal and ex-tramural component; a bulky, irregular mass is common, and
ulceration often occurs (Figure 10-43). Special im-munohistochemical stains are
used to identify the specific tissue types of these neoplasms (ie, c-kit or
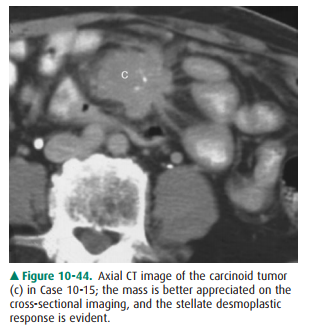
CD117 positiv-ity). Carcinoid tumors arise from enterochromaffin or similar
types of cells, and more than 90% originate in the gastrointestinal tract. Most
carcinoid tumors of the small bowel are located in the ileum. Their radiologic
appear-ances reflect their broad pathologic morphology, and they may present as
single or multiple polypoid lesions or as focal stenosis leading to partial
obstruction; angulation and kinking of bowel loops may occur with a
desmoplastic reaction and cause a mass that is best appreciated on
cross-sectional imaging (Figure 10-44).
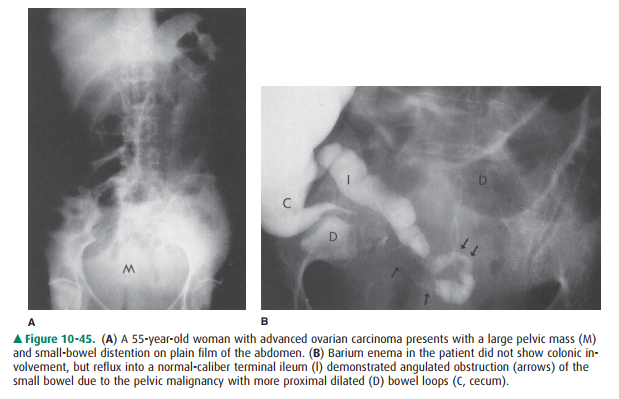
Secondary malignancies involving
the small bowel are much more common than the primary types. The three routes
of secondary malignancy that can spread to the small intestine include (1)
hematogenous metastases, with carcinoma of the breast, lung, and melanoma being
the most common; (2) in-traperitoneal seeding of tumor from elsewhere within
the ab-domen; and (3) direct contiguous invasion of bowel (most often seen with
pancreatic carcinoma and pelvic malignan-cies). Carcinoma of the cervix, endometrium,
and ovary often affects the distal small bowel by intraperitoneal seeding or
di-rect invasion; the colon may also be involved, and radiographic evaluation
of these patients may be best performed with a bar-ium enema, with one goal
being reflux into the ileum (Figure 10-45). Presently, CT and MR imaging of the
abdomen and pelvis have emerged as the usual modalities for assessing and
following patients with intra-abdominal malignancies.
Related Topics