Chapter: Basic Radiology : Gastrointestinal Tract
Exercise: Small-Bowel Bleeding
EXERCISE 10-3.
SMALL-BOWEL BLEEDING
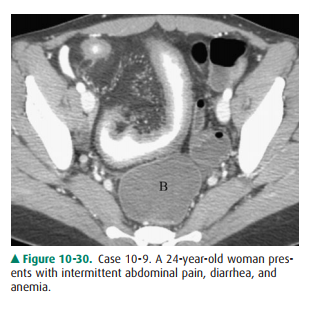
10-9. What is the most likely explanation for the abnormal small-bowel loop anterior to the bladder (B) on this
contrast-enhanced CT examination of the lower ab-domen in Case 10-9 (Figure
10-30)?
A.
Crohn disease
B.
Tuberculosis
C.
Whipple disease
D.
Ulcerated lymphoma
E.
Small-bowel metastases
10-10. What is the
most likely cause of the saccular structure

A.
seen in the distal small bowel in Case 10-10 (Figure 10-31)?
B.
Normal loop of small bowel
C.
Large small-bowel ulcer
D.
Meckel diverticulum
E.
Ulcerated primary malignancy
F.
Small-bowel metastases
10-11. What is the
least likely etiology of the diffuse fold thickening in the central small bowel
in Case 10-11 (Figure 10-32)?

A.
Ischemic enteritis
B.
Small-bowel hemorrhage
C.
Radiation enteritis
D.
Small-bowel edema
E.
Small-bowel malignancy
10-12. What is the
least likely possibility to explain the irregular, ulcerated small-bowel lesion
in Case 10-12 (Figure 10-33)?

A.
Ulcerated GIST
B.
Lymphoma with ulceration
C.
Metastatic ulcerated mass
D.
Large benign ulcer of small bowel
E
Adenocarcinoma with ulceration
Radiologic Findings
10-9. The segmental and enhancing wall
thickening in the ileum is most consistent with
Crohn disease; tuberculosis might appear similar but is rare, and most
neoplasms of the small bowel are focal (A is the correct answer to Question
10-9).
10-10. The smooth,
saccular structure of the small bowel proved to be a bleeding Meckel
diverticulum; benign ulcers of the small bowel are rare, and ulcerated
ma-lignancies are usually irregular in appearance (C is the correct answer to
Question 10-10).
10-11. The long
segment of small bowel of normal caliber with smooth fold thickening (ie,
valvulae con-niventes) suggests submucosal infiltration from fluid (eg, edema
or blood), which may have many causes but not small-bowel malignancy; ischemic
enteritis was the etiology (E is the correct answer to Question 10-11).
10-12. The
irregular, ulcerated mass of the small bowel is typical for an ulcerated
malignancy of various histo-logic types, including metastatic neoplasms; the
cause was a lymphoma (D is the correct answer to Question 10-12).
Discussion
Small-bowel bleeding and
obstruction can be caused by a wide assortment of diseases, some of which may
present with both signs. Crohn disease and ischemia of the small bowel are
likely the two most common causes in younger and older pa-tients, respectively.
Crohn disease is an inflammatory
disorder of the gas-trointestinal tract of unknown etiology. The small bowel
and the ileocecal region are the most common sites of involve-ment. Crohn
disease may affect a single segment, often the terminal ileum, or multiple
areas of the small bowel with normal intervening loops (ie, skip areas). The
involved loop(s) is usually narrowed with a nodular mucosal surface due to
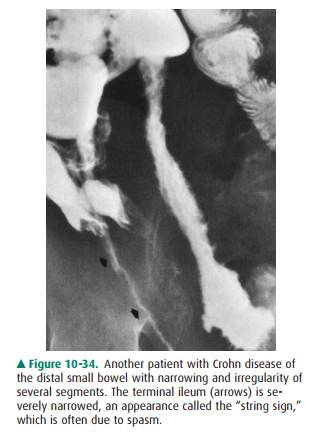
ulceration; deep ulcers and sinus tracts may progress to fistulas. Mark
narrowing of the bowel lumen may relate to active inflammation and spasm with
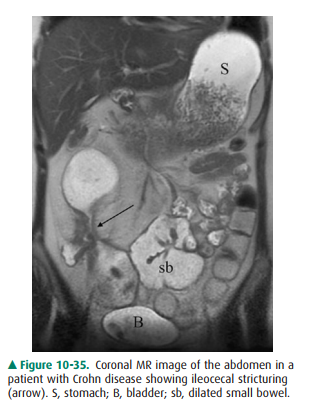
wall thickening or to fi-brotic stenosis (Figure 10-34). CT and MR imaging with
in-travenous contrast enhancement are now commonly used to determine the activity
of Crohn disease and to help with clin-ical management (Figure 10-35).
Meckel diverticulum is one of the
most common anomalies of the gastrointestinal tract and occurs in about 2% to
3% of the population. The diverticulum is usually asymptomatic and is found
incidentally, but may be a cause of intestinal bleeding if the structure
contains ulcerated ectopic gastric mucosa. When shown on radiographic
examination of the small bowel, especially using the enteroclysis technique,
Meckel diverticu-lum appears as a changeable saccular outpouching along the
antimesenteric border of the bowel within a short distance from the ileocecal
junction. A rarer complication of a Meckel diverticulum is inversion into the
lumen of the small bowel with subsequent intussusception and obstruction.
Ischemic disease of the small
intestine can be caused by nonobstructive hypoperfusion of the organ or result
from thrombotic or embolic vascular disease. The radiographic findings are
variable depending on the extent and severity of the underlying process and its
duration. Small-bowel dilatation from ileus or narrowing due to spasm and
sub-mucosal edema and hemorrhage are additional appear-ances; these changes are
also evident on CT and MR imaging, both of which offer further advantages in
assess-ment of the bowel wall, the detection of pneumatosis, and the evaluation
of the mesenteric vessels using CTA or MRA (ie, CT or MR angiography).
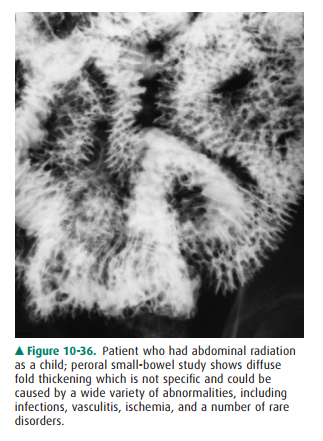
Submucosal infiltration of the small bowel as seen in ischemic enteritis may
occur in other disorders and have similar appearances, such as small-bowel
hemorrhage related to anticoagulants, trauma, hemophilia, or vasculitis;
radiation enteritis is an-other consideration (Figure 10-36). Small-bowel ischemia
may resolve spontaneously or progress to perforation; stricture is a late
complication.
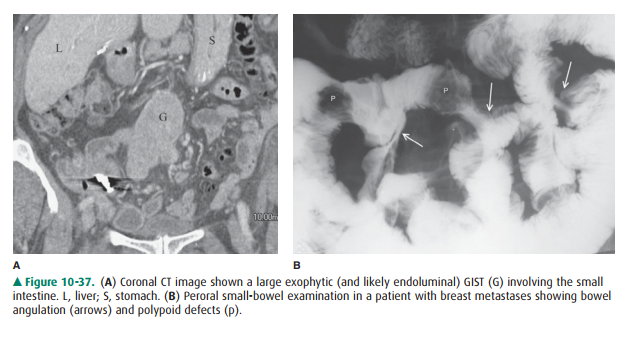
Primary small-bowel neoplasms are
rare. Benign neoplasms of the small intestine are less often symptomatic
compared to malignancies. Adenomas, lipomas, and GISTs/leiomyomas are the most
common benign neoplasms but make up only 60% of the benign total because of a
large number of miscella-neous rarities. Symptomatic small-bowel neoplasms are
usually malignant and nearly all are adenocarcinoma, lym-phoma, carcinoid
tumor, or malignant GIST. These malig-nancies, along with metastatic neoplasms
of the small bowel, show a wide spectrum of appearances varying from polypoid
and ulcerated masses to multifocal and infiltrative processes (Figure 10-37).
Related Topics