Chapter: Basic Radiology : Gastrointestinal Tract
Exercise: Colonic Obstruction
EXERCISE 10-6.
COLONIC OBSTRUCTION
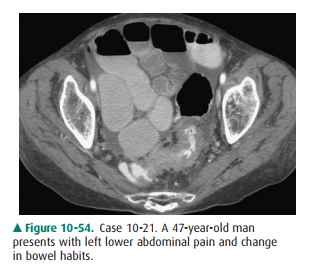
10-21. What is the most likely primary cause of the findings
seen on the pelvic CT examination in Case 10-21 (Figure 10-54)?
A.
Annular carcinoma of descending colon
B.
Ischemic colitis
C.
Small-bowel neoplasm involving colon
D.
Sigmoid diverticulitis
E.
Peritoneal metastases
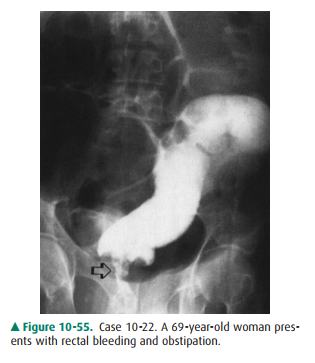
10-22. What is the most likely cause of the irregular, annular
narrowing (arrow) in the lower rectum in Case 10-22 (Figure 10-55)?
A.
Rectal carcinoma
B.
Lymphoma of rectum
C.
Crohn proctitis
D.
Infectious proctitis
E.
Invasive cervical cancer
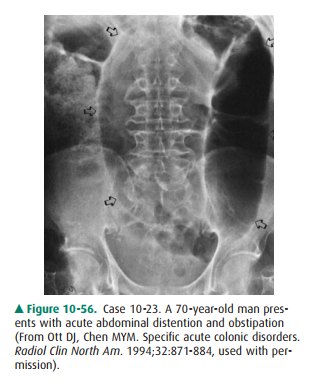
10-23. What is the most likely explanation of the two adja-cent
loops of distended colon (arrows) in Case 10-23 (Figure 10-56)?
A.
Right colon volvulus
B.
Sigmoid volvulus
C.
Ileocecal intussusception
D.
Functional colonic ileus
E.
Internal colonic hernia
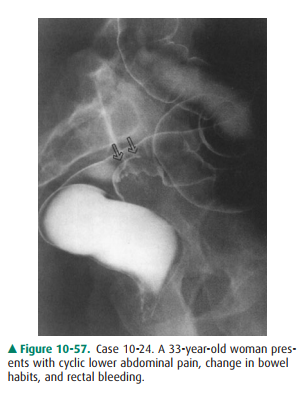
10-24. What is the most likely etiology of the smooth mass
(arrows) partially obstructing the anterior rectosig-moid region in Case 10-24
(Figure 10-57)?
A.
Annular rectosigmoid carcinoma
B.
Rectosigmoid diverticulitis
C.
Pelvic endometriosis
D.
Invasive endometrial carcinoma
E.
Cul-de-sac metastases
Radiologic Findings
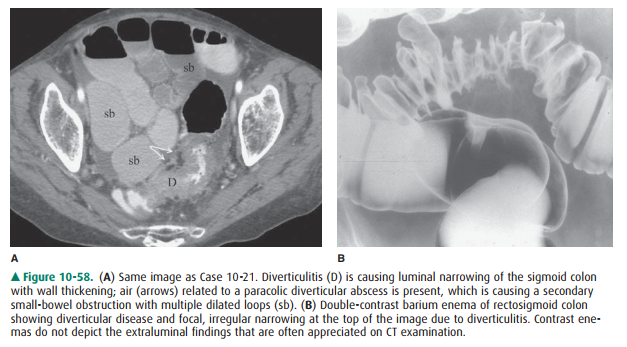
10-21. Sigmoid colon narrowing with adjacent air (Figure 10-58
A, arrows) is present along with secondary small-bowel obstruction related to
diverticulitis (D is the correct answer to Question 10-21).
10-22. An annular rectal carcinoma causing distal colonic
obstruction is present; rectal lymphoma is rare, and the other possibilities
listed do not cause circumfer-ential narrowing of the rectum (A is the correct
an-swer to Question 10-22).
10-23. A sigmoid volvulus is present, which is the most com-mon
colonic volvulus; note the colonic loops point-ing into the sigmoid colon (B is
the correct answer to Question 10-23).
10-24. Pelvic endometriosis is involving the anterior
rec-tosigmoid junction; diverticulitis is rare in this loca-tion, and the
patient is young for the other options offered (C is the correct answer to
Question 10-24).
Discussion
Colonic obstruction when seen in
adults is usually caused by diverticulitis or carcinoma of the colon. Volvulus
of the colonis much less common. However, extrinsic involvement of the rectum
or sigmoid colon from pelvic malignancies is an im-portant consideration in the
middle-aged or older patient.
Diverticulitis is always a
differential consideration in the adult patient with a suspected obstruction of
the distal colon. Diverticulitis is usually due to perforation of a single
diverticulum, with subsequent formation of a paracolic ab-scess, and typically
is located in the sigmoid colon (likely 90% of cases). The radiographic
findings suggesting diverti-culitis on contrast enema of the colon include (1)
extra-vasation into an abscess (the most definitive finding); (2)eccentric or
circumferential narrowing of the colon; and (3)transverse or longitudinal sinus
tracts (also seen in Crohn disease) (Figure 10-58 B). Complications of sigmoid
diverti-culitis are obstruction, fistula formation (especially to the bladder),
and development of a stricture. CT examination of the pelvis has become the
preferred means of evaluating patients suspected of having this disease; the
extramural findings are evident, complications can be identified, and
percutaneous drainage of an abscess can be performed using CT guidance, if
deemed useful clinically.
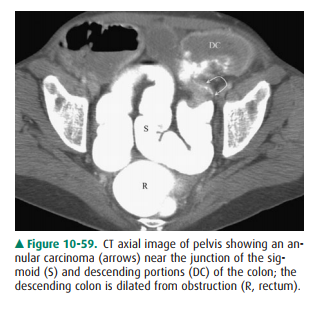
Adenocarcinoma of the colon was
discussed in the previ-ous exercise as a common source of rectal bleeding but
is also an important cause of colonic obstruction. The location and morphologic
type of colonic carcinoma will affect the clinical presentation of the patient.
Carcinomas of the right side ofthe colon are often polypoid, may grow to a
large size, and more often present clinically with localized pain, palpable
mass, and melena. In the left side of the colon, carcinomas usually present at
an earlier stage because obstructive symp-toms are more common, often due to an
annular carcinoma (Figure 10-59). Cross-sectional imaging and CT
colonographyhave assumed a more important imaging role in the detection of
colonic carcinoma, and also in preoperative staging and postoperative
evaluation of patients, especially those with re-current masses; also,
percutaneous biopsy of suspicious areas for possible recurrence can be
performed.
Sigmoid volvulus is a closed-loop
colonic obstruction due to twisting along the mesenteric or long axis of the
bowel. Al-though colonic volvulus is not common, about 90% of cases occur in
the sigmoid colon. On plain abdominal films, the sigmoid volvulus forms an
inverted U-shaped structure with the twisted sigmoid loops lying adjacent and
having an oval appearance called the “coffee bean” sign. On barium enema
examination, tapered obstruction of the sigmoid colon is found (Figure 10-60).
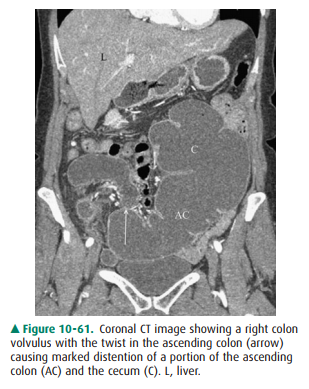
Cecal volvulus results from a twisting obstruction of the right side of the
colon and rarely involves the cecum only (right
colon volvulus is a better term). The di-lated proximal colon may be seen
as an oval structure in the midabdomen or the left upper quadrant, but rarely
points into the pelvis (Figure 10-61). Contrast enemas or CT exam-ination are
used to evaluate patients with potential volvulus of uncertain location; as
with high-grade small-bowel ob-struction, CT examination is often used
initially in patients with possible colonic obstruction.

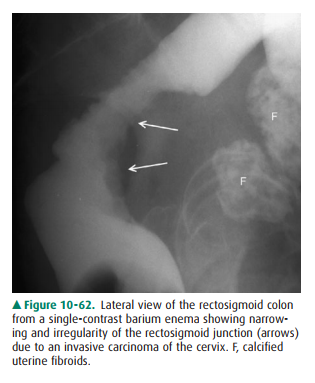
The anterior wall of the
rectosigmoid colon is a common site for involvement of the colon by extrinsic
inflammatory or neoplastic diseases. Inflammatory processes may spread into the
posterior cul-de-sac and secondarily involve the colon; endometriosis can arise
in the same area, implant on the colonic serosa, and invade into the colonic
wall. However, pelvic malignancies related to the uterine cervix, en-dometrium,
ovary, bladder, and prostate are the most com-mon neoplastic processes that can
affect the rectosigmoid colon. Circumferential narrowing may occur with these
ex-trinsic malignances and mimic a primary carcinoma of the colon (Figure
10-62).
Related Topics