Chapter: Basic Radiology : Liver, Biliary Tract, and Pancreas
Exercise: Diffuse Liver Disease
EXERCISE 11-1.
DIFFUSE LIVER DISEASE
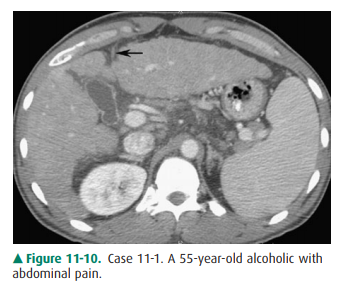
11-1. What is the most likely diagnosis in Case 11-1 (Figure 11-10)?
A.
Cirrhosis
B.
Diffuse liver tumor
C.
Budd-Chiari syndrome
D.
Schistosomiasis
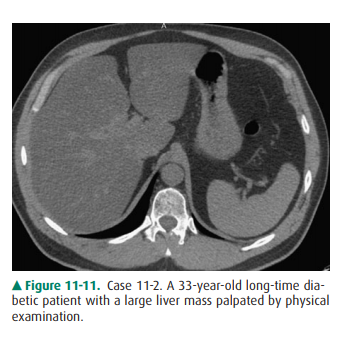
11-2. What is the most likely diagnosis in Case 11-2 (Figure 11-11)?
A.
Cirrhosis
B.
Fatty liver
C.
Hepatic iron overload
D.
Old granulomatous disease
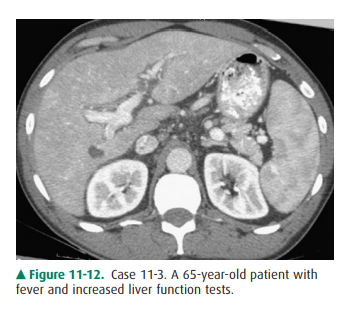
11-3. What is the most likely diagnosis in Case 11-3 (Figure 11-12)?
A.
Cirrhosis
B.
Thorotrast-induced liver disease
C.
Hepatitis
D.
Hepatic iron overload
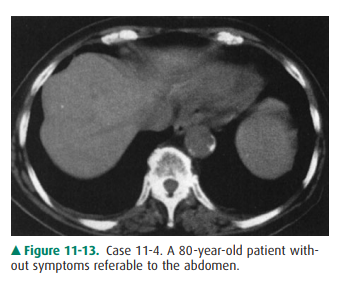
1-4. What is the most likely diagnosis in Case 11-4 (Figure 11-13)?
A.
Cirrhosis
B.
Old granulomatous disease
C.
Fatty liver
D.
Osler-Weber-Rendu disease
Radiologic Findings
11-1. In this case, the overall size of the liver is small. The
contour of the liver is nodular, which is characteristic of cirrhosis. Also
note the recanalized paraumbilical vein (arrow), which indicates portal hypertension
(A is the correct answer to Question 11-1).
11-2. In this case, the liver is enlarged, there is marked low
density throughout the liver when compared with the spleen, and there is no
mass effect on the vessels. These are findings of fatty liver (hepatic
steatosis) (B is the correct answer to Question 11-2).
11-3. In this case, the liver size is enlarged and the liver
demonstrates heterogeneous attenuation through-out. No focal mass is seen.
These findings are consis-tent with hepatitis in this clinical setting (C is
the correct answer to Question 11-3).
11-4. In this case, multiple small, highly attenuating,
punctuate lesions are scattered throughout liver and spleen, characteristic of
calcifications from old granulomatous disease, without any other predom-inant
finding (B is the correct answer to Question 11-4).
Discussion
Differentiation of liver disease
into diffuse or focal disease is an artificial but convenient way to analyze
liver disorders ra-diographically. Diffuse hepatocellular diseases are a common
diagnostic problem. Although historical, physical, and labo-ratory testing are
the first means for identifying these dis-eases, imaging may be required as a
part of the overall assessment of the patient. Cirrhosis is a chronic disease of
the liver. It is character-ized by injury and regeneration of hepatic
parenchymal cells and is accompanied by formation of connective tissue within
the liver. In the United States, the most common cause of cirrhosis is
alcoholism, whereas in Asia, the most common cause is viral hepatitis.
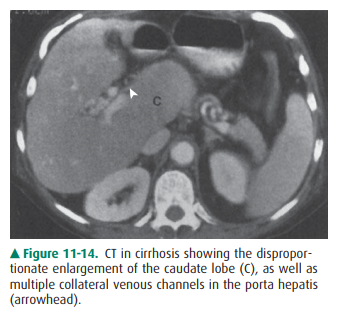
Cirrhosis results in dis-proportionate diminution of the right lobe compared to
the left lobe and caudate lobe of the liver (Figure 11-14). Nodular
regeneration of the liver results in a nodular edge of the liver and inhomogeneity
of the parenchyma. The process is accompanied by, first, increased resistance
to normal hepatopetal (toward the liver) flow and, finally, the development of
hepatofugal (away from the liver) flow. The increased resistance in the portal
vein secondarily en-larges the spleen. This process also creates enlarged
collat-eral venous channels to reroute blood around the liver (Figure 11-10).
These portosystemic collaterals are visible frequently on cross-sectional
imaging studies, most com-monly in paraumbilical veins, coronary veins, and
even spontaneous splenorenal shunts. Ascites is nearly always present. Most
authorities are increasingly convinced that MR imaging is the most sensitive
imaging modality for ex-amination of the liver in cirrhosis and other diffuse
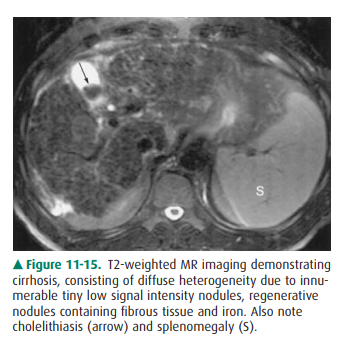
dis-eases of the liver. MR imaging can demonstrate not only the contour changes
and collateral formation visible with CT, but also the more subtle
intraparenchymal nodular changes consequent to formation of regenerative and
dys-plastic nodules characteristic of cirrhosis within the com-plex fibrotic
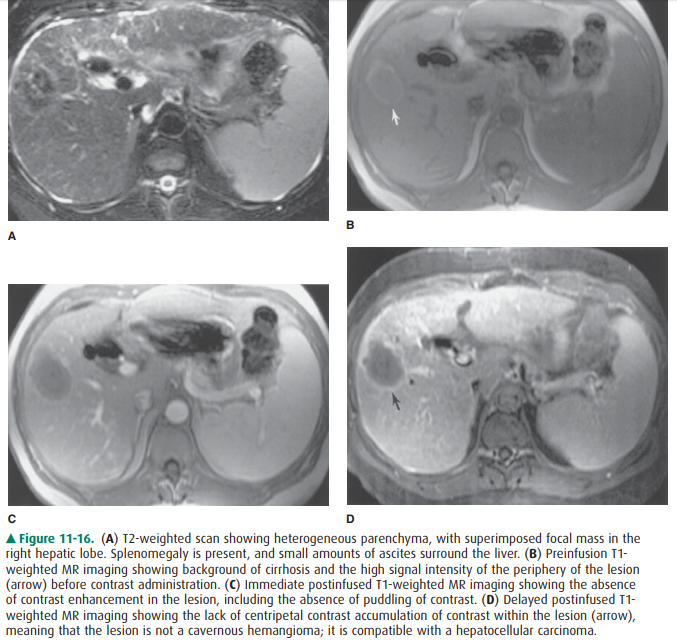
and inflamed host hepatic tissue (Figure 11-15). Importantly, MR imaging is
considered to be a sen-sitive imaging means in the diagnosis of tumors such
ashepatocellular carcinoma superimposed on a background of cirrhosis (Figure
11-16).
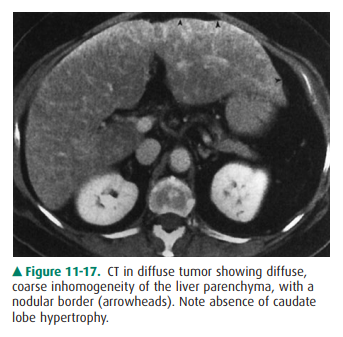
Diffuse tumor in the liver can
occur in patients with cer-tain primary malignancies (Figure 11-17),
particularly breast carcinoma. It is usually distributed randomly throughout
the left and caudate lobes. Collateral veins normally are not found. Portal
venous or intrahepatic biliary radicles may be compromised or displaced,
although portal vein thrombosis is uncommon.
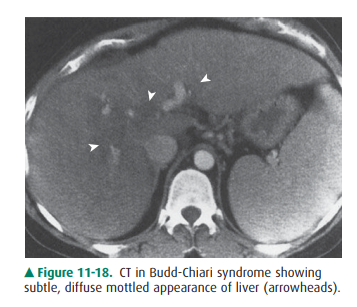
Budd-Chiari syndrome is a
condition involving obstruc-tion of the hepatic veins or the intrahepatic inferior
vena cava. It is due to hypercoagulable states that produce thrombosis; tumors
of the liver, kidneys, adrenal glands, or inferior vena cava (IVC); trauma (the
“three Ts,” ie, throm-bosis, tumors, trauma); pregnancy; and even webs or
membranes in the lumen of the inferior vena cava. This syndrome produces a
marked congestion of the liver result-ing from resistance to flow out of the
liver, which conse-quently enlarges and becomes edematous. The liver has a
mottled appearance on CT that is due to the interstitial edema, especially
after administration of intravenous con-trast material (Figure 11-18).
Schistosomiasis is one of the
world’s most common par-asitic diseases and is rarely seen in persons living
outside the endemic areas of China, Japan, the Middle East, and Africa; it does
occur in immigrants to the United States. The larvae are hosts that enter the
human gastrointestinal system, pass into lymphatic channels, migrate into
mesenteric veins and portal veins, and, as adult worms, deposit ova that
embolize to the portal system. This process leads to a granulomatous
inflammation, periportal fibrosis, portal vein occlusion, varices, and
splenomegaly. Imaging studies demonstrate periportal fibrosis. The fibrosis
enhances on CT after con-trast material administration and appears on US as
in-creased echogenicity of the periportal sheath surrounding the portal veins.
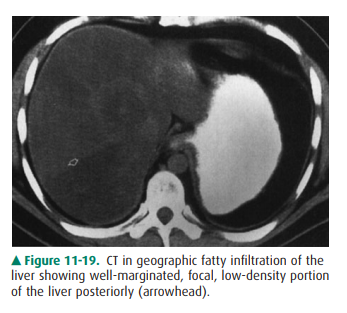
Fatty liver, or steatosis, is a
common disorder. It is found in up to 50% of diabetic and alcoholic patients
and has been found in up to 25% of nonalcoholic, healthy adults who die
accidentally. The many causes of fatty liver, besides diabetes and alcoholism,
include (1) obesity, (2) chronic illness, (3) corticosteroid excess, (4)
parenteral nu-trition, and (5) hepatotoxins, including chemotherapy. Fatty
liver may be distributed evenly or focally. When dis-tributed uniformly, fatty
liver is recognizable as a pattern of homogeneous increased echogenicity on US,
decreased at-tenuation on CT (Figure 11-11), or increased signal inten-sity on
T1-weighted MR images. On ultrasound, the echogenicity of the liver is compared
to the right kidney, whereas on CT, the density of the liver is compared to
thespleen. When distributed nonuniformly, it resembles focal disease of the
liver in that normal islands of liver tissue are seen against the background of
lower-density fatty liver (Figure 11-19). Specialized MR imaging scans such as
chemical shift imaging, NM studies, or biopsy may be re-quired to differentiate
among the possibilities.
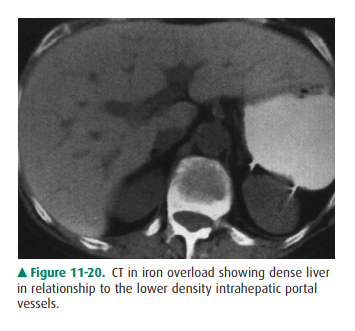
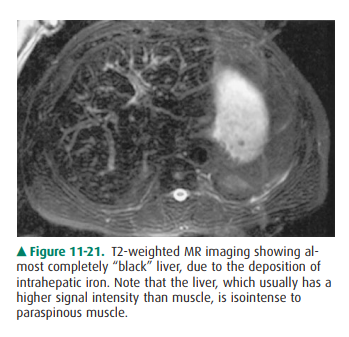
Hepatic iron overload can be due
to deposition in hepato-cytes or reticuloendothelial cells. Parenchymal iron
deposition occurs in primary idiopathic hemochromatosis,
secondaryhemochromatosis, cirrhosis, or intravascular hemolysis; the iron
overload in these conditions is generally referred to as hemochromatosis.
Reticuloendothelial iron deposi-tion occurs in transfusional iron overload or
rhabdomyol-ysis; the iron overload in these conditions is referred to as
hemosiderosis. The liver, including the right lobe, is en-larged greatly unless
cirrhosis is present. On CT, the den-sity of the liver is very high (Figure
11-20), and on MR imaging the liver has extremely low signal on both T1-
andT2-weighted images (Figure 11-21). Patients with hepatic iron overload may
develop hepatocellular carcinoma.
Old granulomatous disease is a
disorder in which prior granulomatous inflammation, usually caused by Histo-plasma capsulatum, involves the
liver. Other granulomatous inflammatory
conditions that could be involved include sarcoidosis, Wegener’s
granulomatosis, and certain toxins. The granuloma tends to undergo necrosis,
and dystrophic calcification forms within the lesion. This gives the lesion its
most characteristic form, multiple punctate calcifica-tions. The granuloma is
visible on US as focal, extremely hyperechoic, shadowing lesions, and on CT as
extremely high-density punctuate lesions (Figure 11-13). When large enough to
be seen on MR, the calcification is seen as a signal void.
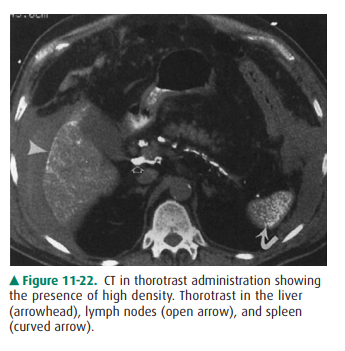
Thorotrast, a thorium-containing
contrast agent, was used in the early 20th century for angiography and other
purposes. Unfortunately, thorotrast emits alpha and beta ra-diation and has a
biologic half-life of 400 years because it is not excreted; it therefore has
been responsible for the devel-opment of several malignancies of the liver and
spleen, in-cluding angiosarcoma and hepatocellular carcinoma. The particles are
taken up by liver, spleen, lymphatics, and bone marrow. They appear on CT
studies as large, dense particles in the liver, spleen, and peripancreatic and
periportal lymph nodes (Figure 11-22). US shows typical calcifications.
Hepatitis is a diffuse
inflammation of the liver, occurring as either acute or chronic disease.
Patients with acute hepati-tis have hepatocellular necrosis. In chronic cases,
periportal inflammation and even fibrosis may occur. In acute hepati-tis, the
echogenicity of the parenchyma is decreased as aresult of the edema, and the
portal radicles are more evident; this has been termed the “starry sky”
appearance. In chronic hepatitis, the texture of the liver is coarsened as a
result of the fibrotic change in the periportal space, and this may de-crease
the visibility of the portal vein radicles. Findings on CT include hepatomegaly
and decreased density (Figure 11-12). Most commonly, no important findings
except hepatomegaly occur on CT in hepatitis. On MR imaging, the liver has low
signal intensity on T1-weighted images and high signal intensity on T2-weighted
images because of the edema and inflammation.
Osler-Weber-Rendu disease, or
hereditary hemorrhagic telangiectasia, affects many organs and is seen
predomi-nantly, but not exclusively, in skin and the gastrointestinal tract. In
the liver, it produces telangiectasias, cirrhosis, or both. Multiple small
aneurysms may be present, and hematomas may occur if the aneurysms bleed. These
aneurysms and any consequent hematomas from aneurysmal rupture can be vis-ible
on both US and CT. Angiography can demonstrate en-larged hepatic arteries and
early but not immediate hepatic vein opacification.
Related Topics