Chapter: Obstetric and Gynecological Nursing : Infection of the Female Reproductive Organs
Ectopic Pregnancy
Ectopic Pregnancy
If the fertilized ovum embeds outside the uterus the condition is known
as an ectopic pregnancy. Most commonly this occurs in the ampulla portion of
the fallopian tube. Other rare implantation sites are the abdomen, cervix,
ovary and fallopian tube portions other than ampulla. The incidence of ectopic
pregnancy is 1 in 150 conceptions.
Causes
Pelvic inflammatory disease as a result of early and indiscriminate
sexual activity.
·
Women who have had tubal surgery
·
Women who have use the IUCD
The right and left fallopian tubes are involved with equal frequency,
and rarely a tubes pregnancy may occur in both tubes.
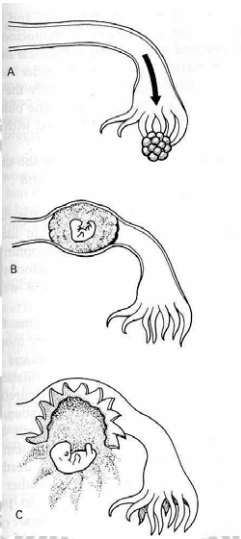
Figure 19. Possible outcomes of a tubal pregnancy. (A) Tubal abortion. (B) Tubal mole. (C) Ruptured tubalpregnancy.
Implantation may occur in the fimbriated (17%); the ampulla (55%), the isthmus (25%) the interstitial portion (2%) and rarely the ovarian 0.5% or the abdominal cavity 0.1%. In most cases the pregnancy terminates between the 6th and 10th weeks of pregnancy.
A. Tubal Pregnancy
The main cause is damage and distortion of the fallopian tubes.
Implantation can occur at any point along the fallopian tube.
Out come of the pregnancy
Tubal abortion
Tubal rupture
Tubal mole
Secondary abdominal pregnancy
Sign and symptoms
Manifests by mild lower abdominal discomfort with an occurrence of sharp
acute attack of stabbing pain accompanied by nausea. This may be sufficiently
severe for the mother to seek medical advice.
Usually there is a short period of amonrrhea in ruptured ectopic
gestation fainting is usual Vaginal breeding may bemistaken for bleeding due to
a delayed menstrual period or an abortion.
Slight brownish color and continuous breeding with rarely present crops.
B. Tubal abortion
This occurs in 65% of the cases and is the usual termination in fimbrial
and ampullary implantation repeated small bleeding from the invaded area of the
tubal wall separated the ovum., which dies and is either aborted completely or
aborted thorough the tubal ostium into the peritoneal cavity or aborted
incompletly so that the clot covered conceptus distends the ostium or forms a
tubal blood mole
C. Tubal rupture
This occurs in 45% of cases, and is more common when the implantation is
in the isthmus. If the implantation is in the isthmus, where the mucosa is
thinner and the vessles are larger, penetration of the muscularity and tubal
rupture occurs earlier and internal hemorrhage is usually sever, which if the
implantation is in the interestial portion of the oviduct, rupture is often
delayed as the myometrium surrounds the growing conceptus; but eventually it
does occur and is attended by sever hemorrhage. The rupture is being sudden or
gradual. Ifthe rupture is on the mesenteric side of the tube, a broad ligament
haematoma will form.
D. Secondary abdominal pregnancy
Very rarely the extruded ovum continious to grow as sufficient
trophoblast maintains its conception with the tubal epithelium and latter the
trophoblast covering the ova sac attaches to abdominal organs. A few of these
pregnancies advance to term and in a few fetus dies early.
Two clinical patterns occur, and are due to the extent of the damage to
the tube wall by the invading trophoblast. The first is sub acute, the second
acute.
Sub acute
After a short period of amenorrhea, the patient complains of:
·
some lower abdominal discomfort, may be so mild
·
occasionally there is an attack of sharp pain and faintness,
·
an attack of sharp pain favored by slight breeding
·
Tenderness of a lower abdomen on examination
·
Vaginal examination show a tender fornix or a vague mass
·
If the patient is observed, further episodes of pain will occur
·
Vaginal bleeding, usually brown in color causing acute collapse
indicating tubal rupture or incomplete tubalabortion or the symptoms could
indicate complete abortion with or without pelvic haematocole.
Acute
Sudden collapse with little or no warning is more common when the
implantation is isthamal, but is not the most frequent events. It is more usual
for the acute tubal rupture to supervene upon the sub acute.
As the tube ruptures
·
The patient is seized with a sudden acute lower abdominal pain,
sufficiently sever to case fainting
·
The associated internal hemorrhage leaders to rapid contapse, with
pallor a week pulse with a rising rate and a falling blood pressure usually the
condition improves after a short time, as the hemorrhage diminishes or cases
but abdominal discomfort persist and pain is felt in the epigastrium and
referred to the shoulder.
·
A further episode of hemorrhage and collapse is likely, and continued
breeding can be suspected from increasing pallor and a falling hemoglobin
level.
·
On examination the patient is shocked, the lower abdomen is tender with
some abdominal muscle guarding
·
Vaginal examination, which should only be carried out in hospital, shows
extreme tenderness in the fornixes and marked tenderness on movement from side
to side.
Diagnosis
·
The presence of internal bleeding in acute cases. An immunological
pregnancy test is positive in 75 % of cases which is not very specific if the
BHCG test is positive, a pelvic ultrasound examination be made.
·
If ultrasound examination shows fetus in the fallopian tube and empty
uterus the diagnosis is certain and a laparotomy should be made If the
diagnosis remains in doubt a laparoscopy will clear the matter up
Treatments
When tubal pregnancy is suspected the patient must be transferred to
hospital with out vaginal examination provided she is not in shock and
intravenous infusion of saline or a plasma expander given.
As soon as the diagnosis of ectopic gestation is made in hospital,
laparatomy should be performed at once, even if the patient is collapsed. Blood
transfusion should be started as soon as after admission as possible.
Prognosis
Only 60 percent of patients who have had an ectopic gestation become
pregnant again. Of the women who do not have a future pregnancy, 75 percent
avoid pregnancy voluntarily, and 75 percent are involuntarily infertile. The
riskof a second ectopic gestation is about 10 percent, as compared which 0.4
percent in other women. The chance of delivering a term baby is about 50
percent. Patients who have previously had an ectopic gestation therefore
require additional care during pregnancy.
Related Topics