Chapter: Medical Physiology: Muscle Blood Flow and Cardiac Output During Exercise; the Coronary Circulation and schemic Heart Disease
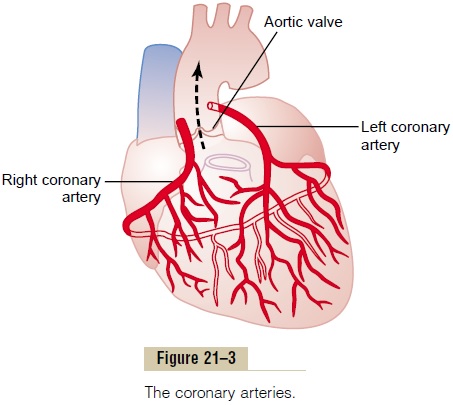
Control of Coronary Blood Flow
Control of Coronary Blood Flow
Local Muscle Metabolism Is the Primary Controller of Coronary Flow
Blood flow through the coronary system is regulated mostly by local arteriolar vasodilation in response to cardiac muscle need for nutrition. That is, whenever the vigor of cardiac contraction is increased, regard-less of cause, the rate of coronary blood flow also increases. Conversely, decreased heart activity is accompanied by decreased coronary flow. This local regulation of coronary blood flow is almost identical to that occurring in many other tissues of the body, especially in the skeletal muscles all over the body.
Oxygen Demand as a Major Factor in Local Coronary Blood Flow Regulation. Blood flow in the coronaries usually is reg-ulated almost exactly in proportion to the need of the cardiac musculature for oxygen. Normally, about 70 per cent of the oxygen in the coronary arterial blood is removed as the blood flows through the heart muscle. Because not much oxygen is left, very little additional oxygen can be supplied to the heart mus-culature unless the coronary blood flow increases. For-tunately, the coronary blood flow does increase almost in direct proportion to any additional metabolic con-sumption of oxygen by the heart.
However, the exact means by which increased oxygen consumption causes coronary dilation has not been determined. It is speculated by many research workers that a decrease in the oxygen concentration in the heart causes vasodilator sub-stances to be released from the muscle cells and that these dilate the arterioles. A substance with great vasodilator propensity is adenosine. In the presence of very low concentrations of oxygen in the muscle cells, a large proportion of the cell’s ATP degrades to adeno-sine monophosphate; then small portions of this are further degraded and release adenosine into the tissue fluids of the heart muscle, with resultant increase in local coronary blood flow. After the adenosine causes vasodilation, much of it is reabsorbed into the cardiac cells to be reused.
Adenosine is not the only vasodilator product that has been identified. Others include adenosine phosphate compounds, potassium ions, hydrogen ions, carbon dioxide, bradykinin, and, possibly, prostaglandins and nitric oxide.
Yet, difficulties with the vasodilator hypothesis exist. First, pharmacologic agents that block or partially block the vasodilator effect of adenosine do not prevent coronary vasodilation caused by increased heart muscle activity. Second, studies in skeletal muscle have shown that continued infusion of adeno-sine maintains vascular dilation for only 1 to 3 hours, and yet muscle activity still dilates the local blood vessels even when the adenosine can no longer dilate them. Therefore, the other vasodilator mechanisms listed above must be remembered.
Nervous Control of Coronary Blood Flow
Stimulation of the autonomic nerves to the heart can affect coronary blood flow both directly and indirectly. The direct effects result from action of the nervous transmitter substances acetylcholine from the vagus nerves and norepinephrine and epinephrine from the sympathetic nerves on the coronary vessels them-selves. The indirect effects result from secondary changes in coronary blood flow caused by increased or decreased activity of the heart.
The indirect effects, which are mostly opposite to the direct effects, play a far more important role in normal control of coronary blood flow. Thus, sympa-thetic stimulation, which releases norepinephrine and epinephrine, increases both heart rate and heart con-tractility as well as increases the rate of metabolism of the heart. In turn, the increased metabolism of the heart sets off local blood flow regulatory mechanisms for dilating the coronary vessels, and the blood flow increases approximately in proportion to the meta-bolic needs of the heart muscle. In contrast, vagal stim-ulation, with its release of acetylcholine, slows the heart and has a slight depressive effect on heart con-tractility. These effects in turn decrease cardiac oxygen consumption and, therefore, indirectly constrict the coronary arteries.
Direct Effects of Nervous Stimuli on the Coronary Vasculature.
The distribution of parasympathetic (vagal) nerve fibers to the ventricular coronary system is not very great. However, theacetylcholine released by parasym-pathetic stimulation has a direct effect to dilate the coro-nary arteries.
There is much more extensive sympathetic innerva-tion of the coronary vessels. We see that the sympathetic transmitter substances norepineph-rine and epinephrine can have either vascular con-strictor or vascular dilator effects, depending on the presence or absence of constrictor or dilator receptors in the blood vessel walls. The constrictor receptors are called alpha receptors and the dilator receptors are called beta receptors. Both alpha and beta receptors exist in the coronary vessels. In general, the epicardial coronary vessels have a preponderance of alpha recep-tors, whereas the intramuscular arteries may have a preponderance of beta receptors. Therefore, sympa-thetic stimulation can, at least theoretically, cause slight overall coronary constriction or dilation, but usually constriction. In some people, the alpha vaso-constrictor effects seem to be disproportionately severe, and these people can have vasospastic myocar-dial ischemia during periods of excess sympathetic drive, often with resultant anginal pain.
Metabolic factors—especially myocardial oxygen consumption—are the major controllers of myocardial blood flow. Whenever the direct effects of nervous stimulation alter the coronary blood flow in the wrong direction, the metabolic control of coronary flow usually overrides the direct coronary nervous effects within seconds.
Related Topics