Chapter: Ophthalmology: Ocular Trauma
Chemical Injuries in Eye
Chemical Injuries
Etiology:
Chemical injuries can be caused by a variety
of substances such asacids, alkalis, detergents, solvents, adhesives, and
irritants like tear gas. Severity may range from slight irritation of the eye
to total blindness.
Chemical injuries are among the most dangerous
ocular injuries. First aid at the site of the accident is crucial to minimize
the risk of severe sequelae such as blindness.
As a general rule, acid burns are less
dangerous than alkali burns. This is because most acids do not act deeply. Acids differ from alkalis in that they cause immediate coagulation necrosis in the superficial
tissue. This has the effect of preventing the acid from penetrating deeper so that
the burn is effec-tively a self-limiting process. However, some acids penetrate
deeply like alka-lis and cause similarly severe injuries. Concentrated sulfuric
acid (such as from an exploding car battery) draws water out of tissue and
simultaneously develops intense heat that affects every layer of the eye.
Hydrofluoric acid and nitric acid have a similar penetrating effect.
Alkalis differ from most acids in that they can penetrate by
hydrolyzingstructural proteins and dissolving cells. This is referred to as liquefactivenecrosis. They then cause
severe intraocular damage by alkalizing theaqueous humor.
Symptoms:
Epiphora, blepharospasm, and severe pain are
the primarysymptoms. Acid burns usually cause immediate loss of visual acuity
due to the superficial necrosis. In alkali injuries, loss of visual acuity often manifests itself only several days
later.
Clinical picture and diagnostic considerations:
Proper diagnosis of thecause and severity of
the burn is crucial to treatment and prognosis.
Alkali burns may appear less severe initially
than acid burns but they lead to blindness.
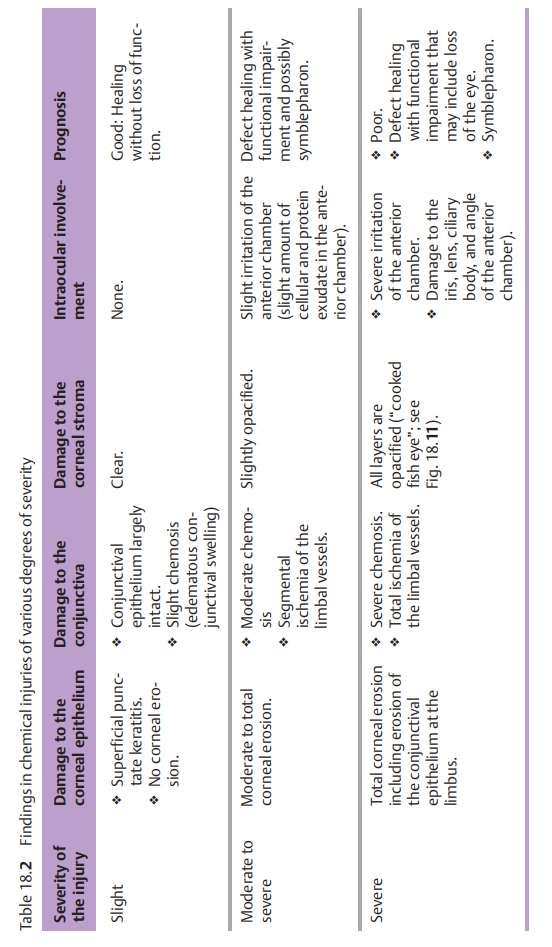
Morphologic findings and the resulting
prognosis can vary greatly depending on the severity and duration of exposure
to the caustic agent. This informa-tion is summarized in Table 18.2.
Treatment:
First aid rendered at the scene of the
accident often decides thefate of the eye. The first few seconds and minutes
and resolute action by per-sons at the scene are crucial. Immediate copious
irrigation of the eye may be performed with any watery solution of neutral pH,
such as tap water, mineral water, soft drinks, coffee, tea, or similar liquids.
Milk should be avoided as it the increases penetration of the burn by opening
the epithelial barrier. A sec-ond person must rigorously restrain the severe
blepharospasm to allow effec-tive irrigation. A topical anesthetic to relieve
the blepharospasm will rarely be available at the scene of the accident. Coarse
particles (such as lime particles in a lime injury) should be flushed and
removed from the eye. Only after these actions have been taken should the
patient be brought to an ophthalmologist or eye clinic.
Chronology of treatment of chemical injuries:
âť– First aid at the scene of the accident (coworkers or family members):
– Restrain blepharospasm by rigorously holding the eyelids open.
– Irrigate the eye within seconds of the
injury using tap water, mineral water, soft drinks, coffee, tea, or similar
liquids. Carefully remove coarse particles from the conjunctival sac.
–
Notify the rescue squad at the same time.
–
Transport the patient to the nearest ophthalmologist or eye clinic.
âť– Treatment by the ophthalmologist or at the eye clinic:
– Administer topical anesthesia to relieve
pain and neutralize blepharospasm.
– With the upper and lower eyelids fully
everted, carefully remove small particles such as residual lime from the
superior and inferior conjuncti-val fornices under a microscope using a moist
cotton swab.
– Flush the eye with a buffer solution.
Long-term irrigation using an irri-gating contact lens may be indicated (the
lens is connected to a cannula to irrigate the eye with a constant stream of
liquid).
–
Initiate systemic pain therapy if indicated.
âť– Additional treatment on the ward in an eye clinic:
The following therapeutic measures for severe
chemical injuries are usu-ally performed on the ward:
–
Continue irrigation.
– Initiate topical cortisone therapy
(dexamethasone 0.1% eyedrops and prednisolone 1% eyedrops).
–
Administer subconjunctival steroids.
– Immobilize the pupil with atropine 1%
eyedrops or scopolamine 0.25% eyedrops twice daily.
– Administer anti-inflammatory agents (two
oral doses of 100 mg indomethacin or diclofenac) or 50 – 200 mg systemic
prednisolone.
–
Administer oral and topical vitamin C to neutralize cytotoxic radicals.
– Administer 500 mg of oral acetazolamide
(Diamox) to reduce intraocu-lar pressure as prophylaxis against secondary
glaucoma.
– Administer hyaluronic acid for corneal care
to promote re-epithelial-ization and stabilize the physiologic barrier.
–
Administer topical antibiotic eyedrops.
– Debride necrotic conjunctival and corneal
tissue and make radial inci-sions in the conjunctiva (Passow’s method) to drain
the subconjunctival edema.
âť– Additional surgical treatment in the presence of impaired wound
heal-ing following extremely severe chemical injuries:
– A conjunctival
and limbal transplantation (stem cell transfer) can replace lost stem cells
that are important for corneal healing. This will allow re-epithelialization.
– Where
the cornea does not heal, cyanoacrylate glue can be used toattach a hard contact lens (artificial
epithelium) to promote healing.
– A Tenon’s capsuloplasty (mobilization and
advancement of a flap of subconjunctival tissue of Tenon’s capsule to cover
defects) can help to eliminate conjunctival and scleral defects.
âť–Late surgical treatment after the eye has stabilized:
– Lysis of symblepharon (symblepharon refers
to adhesions between the palpebral and bulbar conjunctiva; see also prognosis
and complica-tions) to improve the motility of the globe and eyelids.
– Plastic surgery of the eyelids to the
release the globe. This should be only performed 12 to 18 months after the
injury).
– Where there is total loss of the goblet
cells, transplantation of nasal mucosa usually relieves pain (the lack of mucus
is substituted by goblet cells from the nasal mucosa).

– Penetrating keratoplasty may be performed to restore vision. Because
the traumatized cornea is highly vascularized (Fig. 18.10), these procedures are plagued by a high incidence of graft
rejection. A clear cornea can rarely be achieved in a severely burned eye even
with a HLA-typed corneal graft and immunosuppressive ther-apy.
Prognosis and possible complications:
The degree of ischemia of the con-junctiva and
the limbal vessels is an indicator of the severity of the injury and the
prognosis for healing (see Table 18.2).
The greater the ischemia of the
con-junctiva and limbal vessels, the more severe the burn will be. The most
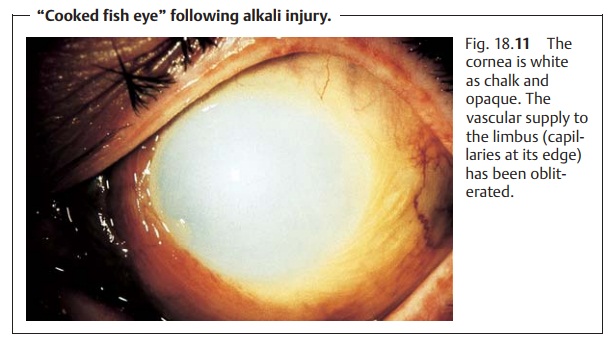
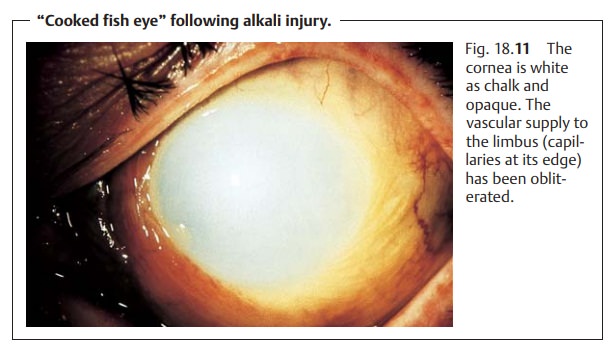
severeform of chemical injury presents as a “cooked fish eye” (Fig. 18.11)
for which the prognosis is very poor, i.e., blindness is possible.
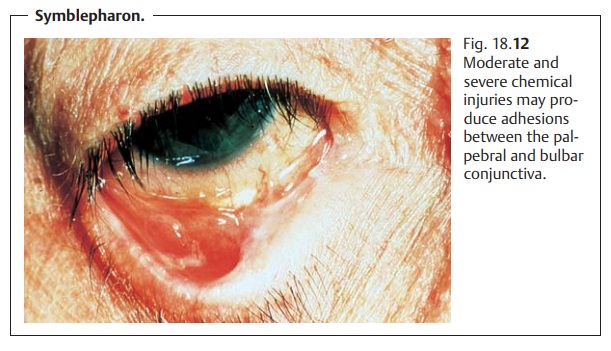
Moderate to severe chemical injuries involving the bulbar and palpe-bral conjunctiva can result in symblepharon (adhesions between the palpebral and bulbar conjunctiva; Fig. 18.12). Inflammatory reactions in the ante-rior chamber secondary to chemical injuries can lead to secondary glau-coma.
Related Topics