Chapter: Biochemical Pharmacology : Some principles of cancer pharmacotherapy
Cell type-specific antitumor drugs
Cell type-specific antitumor
drugs
Among the drugs used in cancer chemotherapy, we
may broadly distinguish two functional groups:
1. Cell-type specific drugs, and
2. General cytotoxic drugs.
The availability of cell type-specific drugs is
limited to se-lected tumours and depends on some specific traits the tu-mour
cells have inherited from their differentiated, healthy ancestors. Most
commonly, this is the dependence of pro-liferation on a particular hormone, or
the the inhibition of growth by a mediator. Examples:
1. Many breast cancers, like normal breast gland
cells, are dependent on estrogens and / or gestagens for their growth. Receptor
antagonists for estrogens (e.g., tamox-ifen) or gestagens (mifepristone, Figure
13.3) will there-fore stop or delay growth of these cells. Of course, these drugs
will affect other hormone-dependent tissues as well – e.g., mifepristone will
also disrupt the function of the placenta in pregnancy, and in fact is used
more com-monly for abortion than for cancer treatment.

2. Hairy-cell leukemia is a rare form of lymphatic4
leukemia. Proliferation of the malignant cells is very ef-ficiently inhibited
by interferon- α. This is one of the few cases so far in which
a `biological' therapy has actually lived up to its promise.
3. Promyelocytic leukemia is caused by a very specific
ge-netic event – the reciprocal translocation of some seg-ments between
chromosomes 15 and 17 (Figure 13.4).
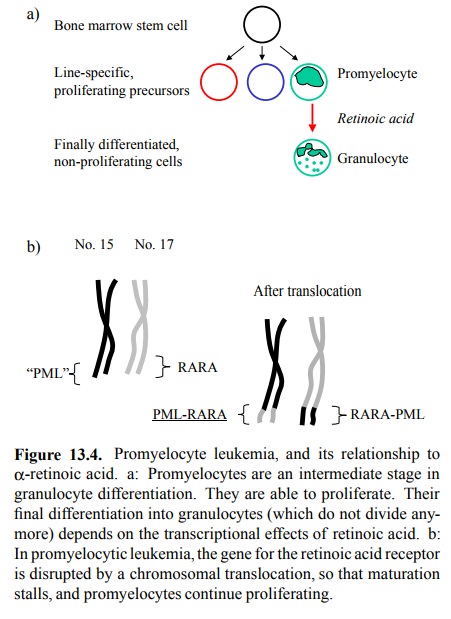
The `rift' of translocation
goes right through the gene for α-retinoic acid receptor, which therefore is
ex-pressed in two deviant forms. Retinoic acid, via its re-ceptors, acts as a
transcriptional regulator in the final differentiation of the promyelocytes to
granulocytes. This differentiation is arrested by the functionally de-viant
receptors. Promyelocytes proliferate, while granu-locytes don't; arrest of
differentiation therefore leads to the build-up of a proliferating yet useless
(even harm-ful) cell population. However, it is possible to restore
differentiation to the aberrant cells by the application of retinoic acid in
larger than physiological amounts. This is probably due to the fact that the
cells are diploid, and the second set of chromosomes 15 and 17 is intact, thus
providing for an intact copy of the α-retinoic receptor gene5.
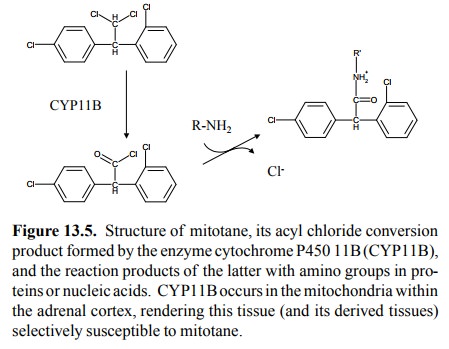
4. Another example of cell type-specific
chemotherapy is the use of mitotane (Figure 13.5) in adrenal gland can-cer
(those derived from the cortex, not the medulla of the adrenal gland).
Selective toxicity is conferred by the enzyme 11-β-hydroxylase, a member of the cytochrome P450
family that is located in the mitochondria of the adrenal gland cortical cells
and participates in the synthesis of glucocorticoids (e.g., cortisone).
Mitotane is a substrate6 for this enzyme, which converts it to an
acyl chloride. The acyl chloride in turn reacts with sever-al proteins in the
mitochondria, which will irreversibly damage the cells.
Importantly,
with all of the above cell-specific therapies, resistance is common, either
primarily (no response to be-gin with) or secondarily (initial response but
emergence of non-responsive cell clones). These therapies therefore typically
have to be combined or followed up with one of the general, non-cell-specific
cytotoxic therapies described below.
Related Topics