Chapter: Pathology: Central Nervous System Pathology
CNS Tumors
CNS TUMORS
CNS
tumors account for 20% of all pediatric tumors. Most pediatric tumors
mainly arise in the posterior fossa, while adult
tumors arise in the supratentorial region. Factors determining prognosis and
response to therapy include the following:
•
Age
•
Tumor location
•
Grade
•
Extent of surgical resection
•
Molecular subgroupings
The World Health Organization
(WHO) grading system assigns grades I–IV, with grade IV tumors the most
aggressive. While grade IV glioblastoma patients usually succumb to disease
within a year, other patients with treatable grade IV tumors may survive 5
years. Metastasis of CNS tumors is rare.
Tumors of Neuroepithelial Tissue
Tumors of neuroepithelial
tissue are categorized as astrocytic tumors, oligoden-droglial tumors,
ependymal tumors, and embryonal tumors (further broken down as medulloblastoma
or CNS primitive neuroectodermal tumor).
Astrocytoma originates from
astrocytes and exhibits fibrillary background, immu-noreactivity for glial
fibrillary acidic protein (GFAP), and diffuse (ill-demarcated) pattern of growth.
•
Pilocytic astrocytoma is a well-differentiated, benign astrocytic
tumor that arises throughout the neuraxis; it is common in children and young
adults. It is the most common benign CNS tumor in children.
•
Sites of involvement include posterior fossa (cerebellum) and
diencephalon
Radiographically, most show
cystic lesion with a mural nodule
Histology shows spindly
neoplastic astrocytes with long bipolar pro-cesses
Rosenthal fibers are thick,
corkscrew-like eosinophilic structures that derive from hypertrophic processes
of astrocytes
Posterior fossa tumors have
favorable prognosis
Activating mutations in BRAF
are common
•
Fibrillary (diffuse) astrocytoma is a low-grade tumor that arises
in the cerebral hemisphere of young to middle-aged adults and the brainstem of
children.
IDH1 (immunostain) is
positive.
•
Anaplastic astrocytoma is cellular, pleomorphic and mitotically
active.
•
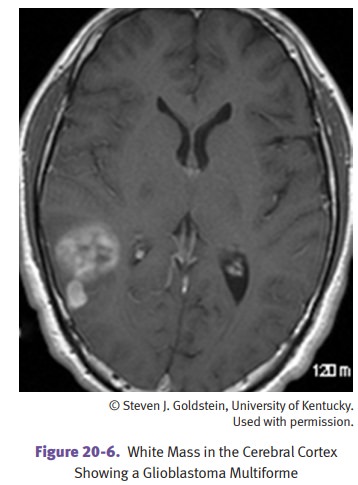
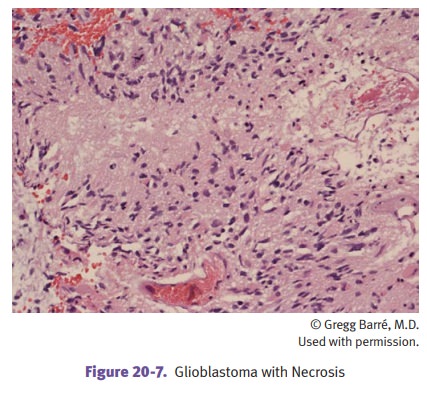
Glioblastoma is the most common CNS primary malignancy in adults.
Histology shows necrosis
and/or vascular proliferation in addition to features seen in anaplastic
astrocytoma.
The prognosis of astrocytomas
varies.
•
Well-differentiated astrocytomas grow slowly; affect younger
patients.
•
Anaplastic astrocytomas and glioblastoma are aggressive; affect
older patients; median survival for glioblastoma is 15 months.
Oligodendroglioma occurs more often in adults
than in children. Its cortical location may cause seizures.
Histologically, perinuclear halos are a fixation artifact that is not seen on
frozen section. This tumor is slow-growing. Tumors with deletions of 1p and 19q
respond well to therapy.
Ependymoma is typically located in the fourth ventricle in
children, where it presents with obstructive
hydrocephalus. In adults the spinal cord is the most common site.
Pseudorosettes are a helpful diagnostic feature on microscopic study.
Multifocality in the spinal cord is associated with NF2. The prognosis depends
on tumor location and adequacy of resection.
Embryonal (primitive) tumors are a group of small round
cell tumors that occur predominantly in children. In
the cerebellum, they are called medulloblastoma.
•
Medulloblastoma is the most common malignant brain tumor in
children.
•
Molecular subgroupings are proving useful for prognosis; Wnt
subgroup has the best prognosis.
Tumors of Cranial and Paraspinal Nerves
Schwannoma originates from Schwann cells of cranial or
spinal nerves. The most frequent location is on CN 8
at the cerebellopontine angle (CPA). Schwannoma manifests characteristically
with unilateral loss of hearing and tinnitus. The prog-nosis is good after
surgical resection.
•
Has spindly cells arranged in hypercellular Antoni A areas;
alternating hypocellular Antoni B areas; and Verocay bodies, parallel rows of neoplastic Schwann cells.
•
Neoplastic cells are immunoreactive for S-100.
Tumors of the Meninges
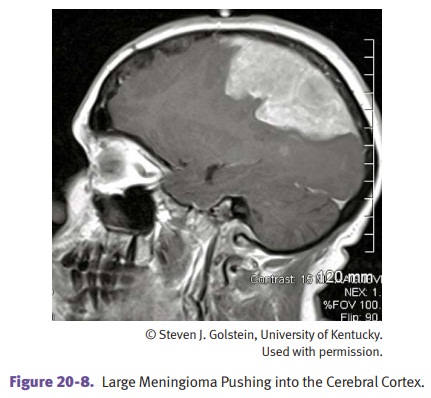
Meningioma is a tumor that originates from meningothelial
cells of the arachnoid. It is common in adults (women
> men) and rare in children. It is a dura-based mass that can recur if the
brain has been invaded, but invasion is unusual. It has varied clinical
features but commonly presents with headache, seizures, and neurological
deficits.
•
Histology shows cellular whorls and psammoma bodies. Many patterns
are seen; the syncytial pattern is common.
•
Abnormalities of chromosome 22 are sometimes present.
•
Multiple meningiomas occur in NF2 patients.
The prognosis of meningioma
is good, though tumors in some locations may not be amenable to complete
resection.
Tumors of the Sellar Region
Craniopharyngioma arises from rests of
odontogenic epithelium within the suprasel-lar/diencephalic region. It most
commonly affects children and young adults. The most common presenting symptoms
are headache, hypopituitarism, and visual field disturbances.
•
Contains deposits of calcium, evident on x-ray
•
Histology shows squamous cells and resembles adamantinoma, a bone tumor of unknown histological origin that is
the most common tumor of the tooth
•
Is benign but tends to recur after resection
•
Beta-catenin (CTNNB1)
gene mutations have been reported
Other Neoplasms
•
Lymphomas
are the
most common CNS tumors in the immunosuppressed. Primary CNS lymphomas may be
multiple, unlike other histologic types. They do not respond well to
chemotherapy.
•
Germ
cell tumors are more common in children than adults. The germinoma is the most common histologic type. It resembles
the seminoma of the testis and the dysgerminoma of the ovary; the cells are
large with a prominent nucleolus. These tumors are radiosensitive.
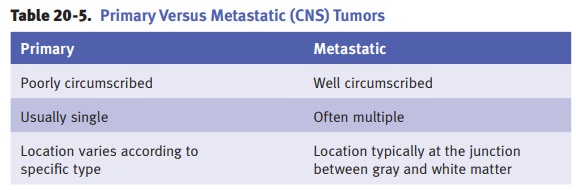
Metastatic Tumors
About 25–50% of all CNS
tumors are metastatic tumors from sources outside the CNS. Carcinomas are the most common.
Related Topics