Chapter: Pathology: Central Nervous System Pathology
Cerebrovascular Disease
CEREBROVASCULAR DISEASE
Cerebrovascular disease is the third most frequent
cause of death in industrialized countries, and it is the
leading cause of serious disability in the United States. Risk factors are
similar to coronary artery disease.
•
Global
cerebral ischemia (diffuse ischemic encephalopathy) is caused by a fall in blood flow to the brain, due to processes
such as shock, cardiac arrest, and hypotensive episodes. While the entire brain
can be damaged, some regions have selective vulnerability, including Purkinje
neurons, hippocampus, CA1 (Sommer sector), and pyramidal neurons of cortex. The
pathology often includes infarcts in watershed areas, cortical laminar
necrosis, and diffuse ischemic necrosis of neocortex. Global cerebral ischemia
may lead to brain death.
•
Transient
ischemic attack (TIA) is due to small platelet thrombi or athero-emboli and is
characteristically reversible, with symptoms lasting less than 24 hours.
•
Stroke can be due to infarction (85%
of all stroke cases) or hemorrhage (15% of all stroke cases).
•
Infarction causes 85% of all stroke cases.
Can be due to thrombotic
occlusion in the setting of atherosclerosis of the cerebral arteries; the
thrombotic infarction is characteristically an anemic (white) infarct.
Can be due to embolic
occlusion, most often due to thromboemboli from cardiac chambers and less
frequently due to atheroemboli. Embolic infarction produces a hemorrhagic
infarct. Small-vessel disease is a cause of small, lacunar infarcts or lacunae,
and it is related to hypertension, resulting in hyaline arteriolosclerosis.
Atherosclerotic aneuryms are fusiform, involve
the basilar arterty, and present with infarction.
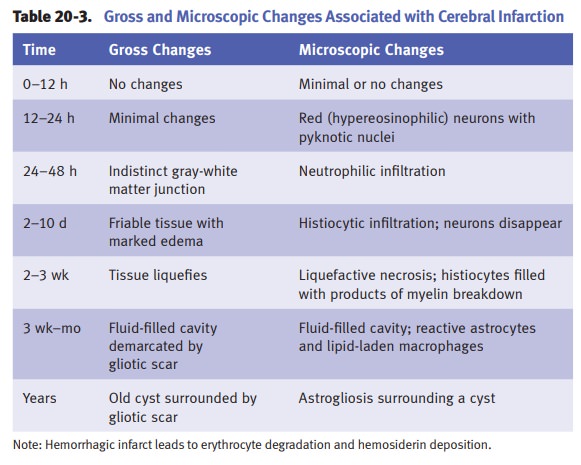
The pathology (i.e.,
morphological features of brain infarcts) of infarc-tion is illustrated in
Table 20-3. Clinical manifestations depend on the affected arterial
distribution.
Hemorrhage causes 15% of strokes.
Intracerebral (intraparenchymal) hemorrhage causes severe headache,
fre-quent nausea/vomiting, steady progression of symptoms over 15–20 minutes,
and coma. It is most frequently due to hypertension, and in those instances, it
most commonly involves the basal ganglia, cerebellum, pons, and centrum
semiovale.
Other causes include vascular
malformations (especially arteriovenous mal-formations), cerebral amyloid
angiopathy, neoplasms, vasculitides, abnormal hemostasis, hematological
malignancies, infections, and diabetes mellitus.
Subarachnoid hemorrhage is
most frequently caused by ruptured berry aneu-rysm. Less frequent causes
include extension of an intracerebral or subdu-ral hematoma, vascular
malformations, trauma, abnormal hemostasis, and tumors. Subarachnoid hemorrhage
causes sudden headache (“worst headache of my life”), nuchal rigidity,
neurological deficits on one side, and stupor.
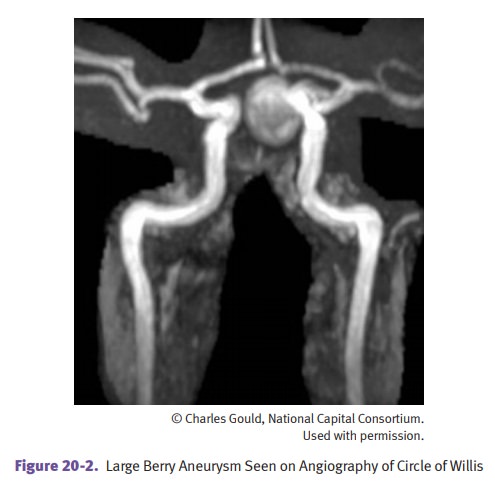
Berry aneurysms are
thin-walled saccular outpouchings, consisting of intima and adventitia only.
They are the most frequent cause of subarachnoid hemorrhage. The most frequent
sites are the anterior circle of Willis at branching points. Rupture is precipitated
by a sudden increase in blood pressure; the prognosis after rupture is that
one-third die, one third recover, and one-third rebleed. The pathogenesis
involves a congenital focal weakness of vessel media that is not identifiable
at birth.Associated disorders include Marfan syndrome, Ehlers-Danlos type 4,and
adult polycystic kidney disease. Hypertension and cigarette smoking predispose
to formation.
Related Topics