Chapter: Essentials of Psychiatry: Childhood Disorders: The Autism Spectrum Disorders
Autism Spectrum Disorders: Differential Diagnosis
Differential Diagnosis
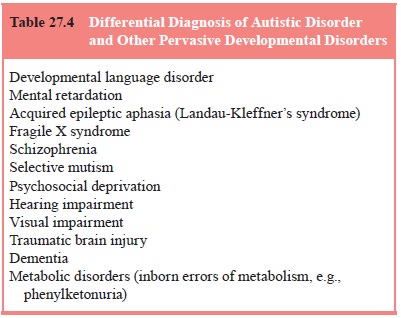
There may initially be some difficulty in
differentiating ASD from other syndromes (Table 27.4), especially in the
context of considerable comorbidity. Mental retardation commonly occurs in ASD,
and children with mental retardation may present with stereotyped movements or
obsessiveness. However, the child with mental retardation and not with ASD will
have social and communicative skills commensurate with their level of overall
development.
Differentiating ASD from childhood schizophrenia is
not usually difficult. The onset of psychosis in childhood is extraor-dinarily
rare, and hallucinations and delusions are not a part of the ASD picture. It is
important not to diagnose some of the atypical features in ASD as psychotic and
equally important to recognize that verbal patients with ASD have impaired
language that should not be confused with schizophrenia. Selective mutism
can be differentiated by the child’s ability to
interact normally in some environments.
Children exposed to severe neglect can sometimes
present with symptoms that look like ASD, but these symptoms will usu-ally show
dramatic improvement when the child is in a more ap-propriate environment.
Perhaps the most difficult differentiation is in a
child with severe obsessive–compulsive disorder (OCD) who also has unu-sual
interests and is inflexible to changes in routines or transi-tions to a new
activity. It is even further complicated if attentional problems coexist. In
these cases, it is important to emphasize the social difficulties of children
with ASD; even if the child with OCD is difficult interpersonally, his or her
ability to maintain eye contact, interpret social situations and emotions and
otherwise interact socially is relatively preserved.
Related Topics