Chapter: Clinical Anesthesiology: Clinical Pharmacology: Adjuncts to Anesthesia
Aspiration: H1-Receptor Antagonists
H1-Receptor Antagonists
Mechanism of Action
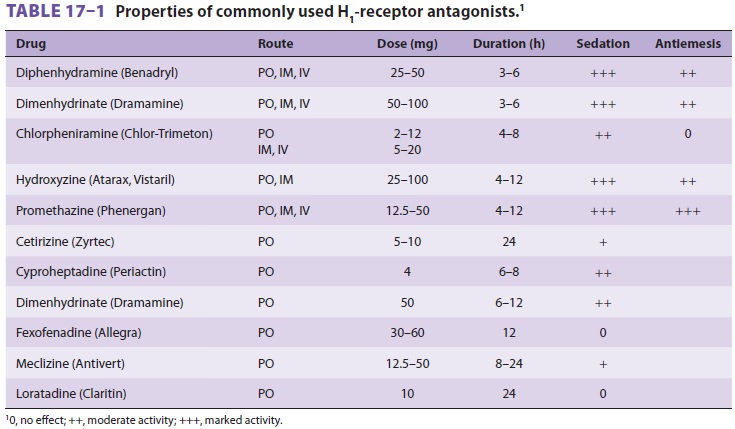
Diphenhydramine (an ethanolamine) is one
of a diverse group of drugs that competitivelyblocks H1 receptors (Table 17–1). Many drugs with
H1-receptor
antagonist properties have considerable antimuscarinic, or atropine-like,
activity (eg, dry mouth), or antiserotonergic activity (antiemetic).
Promethazine is a phenothiazine derivative with H1-receptor
antagonist activity as well as antidopami-nergic and α-adrenergic–blocking properties.
Clinical Uses
Like other H1-receptor antagonists, diphenhydr-amine has a
multitude of therapeutic uses: suppres-sion of allergic reactions and symptoms
of upper respiratory tract infections (eg, urticaria, rhinitis,
conjunctivitis); vertigo, nausea, and vomiting (eg, motion sickness, Ménière’s
disease); sedation; sup-pression of cough; and dyskinesia (eg, parkinson-ism,
drug-induced extrapyramidal side effects). Some of these actions are
predictable from an understanding of histamine physiology, whereas others are
the result of the drugs’ antimusca-rinic and antiserotonergic effects (Table
17–1). Although H1 blockers prevent the
bronchocon-strictive response to histamine, they are ineffective in treating
bronchial asthma, which is primar-ily due to other mediators. Likewise, H1 blockers will not completely prevent the
hypotensive effect of histamine unless an H 2
blocker is administered concomitantly.
The antiemetic and mild hypnotic effects
of antihistaminic drugs (particularly diphenhydr-amine, promethazine, and
hydroxyzine) have led to their use for premedication. Although many H 1 blockers cause significant sedation, ventilatory
drive is usually unaffected in the absence of other sedative medications.
Promethazine and hydroxyzine were often combined with opioids to potentiate
analge-sia. Newer (second-generation) antihistamines tend to produce little or
no sedation because of limited penetration across the blood–brain barrier. This
group of drugs is used primarily for allergic rhini-tis and urticaria. They
include loratadine, fexofena-dine, and cetirizine. Many preparations for
allergic rhinitis often also contain vasoconstrictors such as pseudoephedrine.
Meclizine and dimenhydrinate are used primarily as an antiemetic, particularly
for motion sickness, and in the management of ver-tigo. Cyproheptadine, which
also has significant serotonin antagonist activity, has been used in the
management of Cushing’s Disease, carcinoid syn-drome, and vascular (cluster)
headaches.
Dosage
The usual adult dose of diphenhydramine
is 25– 50 mg (0.5–1.5 mg/kg) orally, intramuscularly, or intravenously every
4–6 h. The doses of other H1-receptor antagonists are listed in
Table 17–1.
Drug Interactions
The sedative effects of H1-receptor antagonists can potentiate other central
nervous system depressants such as barbiturates, benzodiazepines, and opioids.
Related Topics