Chapter: Clinical Anesthesiology: Anesthetic Management: Anesthesia for Patients with Endocrine Disease
Anesthesia for Hyperparathyroidism
HYPERPARATHYROIDISM
Clinical Manifestations
Causes of primary hyperparathyroidism include parathyroid adenomas,
hyperplasia of the para-thyroid gland, and certain
carcinomas. Secondary hyperparathyroidism is an adaptive response to
hypocalcemia produced by conditions such as kid-ney failure or intestinal
malabsorption syndromes. Ectopic hyperparathyroidism is due to production of
PTH by rare tumors outside the parathyroid gland. Parathyroid hormone–related
peptide may cause significant hypercalcemia when secreted by a carci-noma (eg,
bronchogenic [lung] carcinoma or hepa-toma). Bone invasion with osteolytic
hypercalcemia may complicate multiple myeloma, lymphoma, or leukemia. Overall,
the most common cause of hyper-calcemia in hospitalized patients is malignancy.
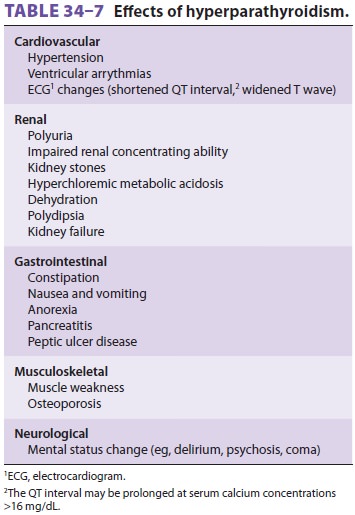
Nearly all clinical manifestations of hyperparathy-roidism are due to
hypercalcemia (Table 34–7). Rarer causes of hypercalcemia include bone
metas-tases of solid organ tumors, vitamin D intoxication, milk-alkali
syndrome, lithium therapy, sarcoidosis, and prolonged immobilization. The
treatment of hyperparathyroidism depends on the cause, but sur-gical removal of
all four glands is often required in the setting of parathyroid hyperplasia.
When there is a single adenoma, its removal cures many patients with sporadic
primary hyperparathyroidism.
Anesthetic Considerations
In patients with hypercalcemia due to hyperpara-thyroidism, hydration with normal saline and diure-sis facilitated by furosemide will usually decrease serum calcium to acceptable values (<14 mg/dL, 7 mEq/L, or 3.5 mmol/L). More aggressive therapy with the intravenous bisphosphonates pamidronate (Aredia) or etidronate (Didronel) may be neces-sary for patients with hypercalcemia of malignancy.
Plicamycin (Mithramycin), glucocorticoids,
calcito-nin, or dialysis may be necessary when intravenous bisphosphonates are
not sufficient or are contraindi-cated. Hypoventilation should be avoided, as
acidosis increases ionized calcium. Elevated calcium levels can cause cardiac
arrhythmias. The response to NMBs may be altered in patients with preexisting
muscle weakness caused by the effects of calcium at the neuromuscular junction.
Osteoporosis worsened by hyperparathyroidism predisposes patients to vertebral
compression and bone fractures during anesthetic procedures, positioning, and
transport. The notable postoperative complications of parathyroidectomy are
similar to those for subtotal thyroidectomy.
Related Topics