Chapter: Medicine and surgery: Nervous system
Acute confusional state (delirium) - Disorders of consciousness and memory
Acute confusional state (delirium)
Definition
Rapid onset of global but fluctuating confusion with an underlying toxic, vascular, ictal (seizure) or metabolic defect.
Aetiology
Predisposing factors: The very young and very old, hearing loss or visual difficulty, those with diffuse brain disease such as dementia or taking drugs with anticholinergic properties such as tricyclic antidepressants, unfamiliar environment (e.g. hospital, nursing home).
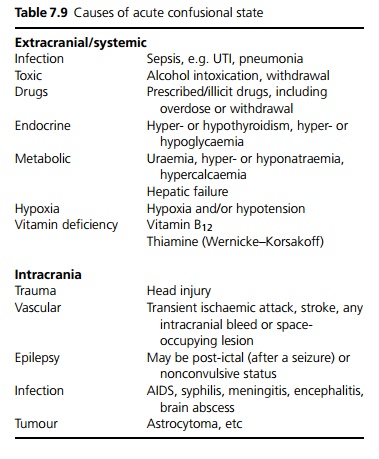
Precipitating factors can be divided into intracranial and extracranial (see Table 7.9).
Clinical features
Disorientation and impaired conscious level – especially worse at night.
Poor cognition, incoherent thought and speech.
Mood and affect labile with depression, irritability, paranoia and aggression.
Hallucinations – auditory and visual. Delusions are common.
Motor activity may be increased but is often purposeless.
Autonomic overactivity: Sweating, tachycardia and dilated pupils.
A detailed history including premorbid cognitive state, alcohol and drugs is essential, fluctuation helps separate delirium from dementia, examination should look for focal neurological signs and any evidence of other illness. Patients with dysphasia may appear confused, and require careful assessment.
Investigations
Blood: FBC, U&E, ESR, CRP, calcium, glucose, thyroid function, syphilis serology, LFTs and clotting screen.
Blood cultures if pyrexial.
Urine for microscopy and culture. Consider saving urine for toxicology screen.
ECG for possible acute myocardial infarction, arrhythmia, signs of hyperkalaemia.
Imaging includes CXR, and where indicated CT or MRI.
Management
Detection of the underlying cause of the confusional state and relevant treatment.
Supportive therapy including rehydration, correction of electrolyte imbalance, improved lighting at night, facilitation of orientation, and avoidance of conflict.
Cautious use of shortacting sedatives may be useful for restlessness and agitation, but can exacerbate the problem. Severe cases may require benzodiazepines, haloperidol or one of the newer antipsychotics such as risperidone or olanzapine.
Prognosis
Where recovery occurs it is usually rapid with return to a premorbid functional level. The prognosis is dependent on the underlying cause and comorbid features.
Related Topics