Chapter: Medicine and surgery: Nervous system
Dizziness and vertigo - Clinical Symptoms
Dizziness and vertigo
Vertigo is defined as a hallucination of movement. It is the sensation experienced when getting off a round-about and as part of alcohol intoxication. Patients may complain of dizziness, giddiness, nausea, vomiting and finding standing and walking impossible.
Vertigo may result from peripheral lesions (disease of the labyrinth or the vestibular component of the VIIIth nerve), or central lesions (brain stem). In both types motion, particularly of the head, can exacerbate the sensation. With a chronic lesion such as a tumour, adaptive mechanisms reduce the sensation of dizziness over a period of weeks.
Labyrinth disorders (peripheral lesions)
Peripheral lesions tend to cause a unidirectional horizontal nystagmus enhanced by asking the patient to look in the direction of the fast phase. When the patient walks, they tend to veer to one side, but walking is generally preserved except in the acute stages (see Table 7.2).
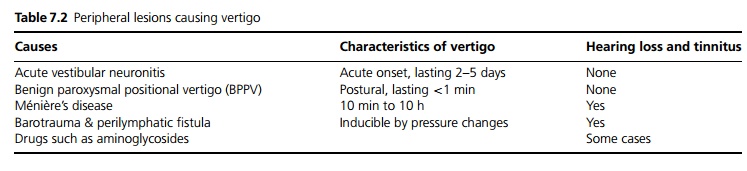
Vestibular neuronitis (acute labrynthopathy) – The most common cause of acute vertigo with nystagmus but without tinnitus or hearing loss. The cause is not known. Symptoms last days to weeks and can be reduced with vestibular sedatives (useful only in the short term), but may recur.
Positional vertigo – vertigo and nystagmus lasting a few seconds which is prompted by head movement. One type is benign paroxysmal positional vertigo (BPPV) which may follow vestibular neuronitis
The Hallpike manoeuvre (see Fig. 7.1): The patient is swung rapidly from a sitting position to lying with the neck extended and turned to one side (so that the head hangs over the end of the bed). The patient’s eyes are closely observed for nystagmus for up to 30 seconds, then sat upright and nystagmus looked for again. This is repeated on the other side. This test can provoke intense nausea, vertigo and even vomiting, particularly in peripheral lesions. In BPPV nystamus
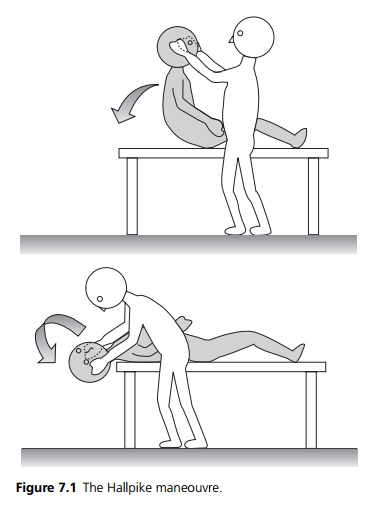
appears after a few seconds (latency), lasts less than 30 seconds (transience), and disappears with repeated testing (fatigable).
Any atypical features suggest a central lesion.
Meni´ere’s` disease is a triad of episodic vertigo lasting a 10 minutes to 10 hours, tinnitus and hearing loss. It responds poorly to vestibular sedatives.
Central lesions
A central lesion due to disease of the brainstem, cerebellum or cortex should be suspected if the history and examination are atypical for a peripheral lesion. For example, risk factors for cerebrovascular disease, previous history of migraine, demyelination, or the presence of any other neurology. Deafness and tinnitus do not occur with central lesions.
Causes include multiple sclerosis, migraine, stroke particularly cerebellar infarction or haemorrhage, vertebrobasilar ischaemia (posterior circulation TIA), tumour of the cerebellopontine angle, cerebellum, fourth ventricle or acoustic neuroma.
Related Topics