Chapter: Medicine and surgery: Nervous system
Coma - Disorders of consciousness and memory
Coma
Definition
Coma is a state of unrousable unconsciousness.
Aetiology
The causes are mainly those of acute confusional state (see Table above), although there are other causes as well. Examples include:
Systemic causes such as hypoglycaemia, hypothyroidism, hypoadrenalism, hypopituitarism,
Intracranial causes such as stroke, space-occupying lesions or haemorrhage tend not to cause coma unless there is extensive cerebral involvement or brainstem involvement (either directly or by raised intracranial pressure).
Clinical features
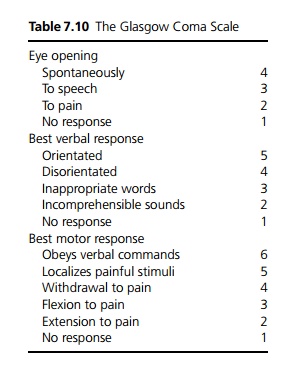
It is important to establish the level of consciousness. A useful way of grading this is the Glasgow Coma Scale (GCS – see Table 7.10).
1 The first priority is resuscitation – stabilise airway, breathing and circulation and check the glucose level (BM). Hypoxia, hypoglycaemia or hypotension are reversible causes of coma and will exacerbate any other cause. If the GCS is ≤8 the patient is at increased risk of aspiration because they are unable to protect their airway, thus intubation and ventilation should be considered.
2 Examination of the patient for clues to a systemic cause, e.g. needle-marks in intravenous drug users, evidence of liver failure, abnormal rate or pattern of respiration and evidence of an intracranial cause, e.g. external evidence of head injury, meningism (meningitis, subarachnoid haemorrhage) and neurological signs.
Investigations
These are as for acute confusional state. In many cases, if early assessment and investigations do not suggest a systemic cause, urgent CT brain is indicated, followed by lumbar puncture if the CT scan is normal.
Management
Following resuscitation treatment of the underlying cause is the main priority.
If hypoglycaemia is possible, intravenous glucose should not be delayed. In at-risk patients such as alcoholics and in pregnancy, intravenous thiamine should be given prior to any intravenous glucose as there is a small risk of precipitating irreversible Wernicke– Korsakoff ’s syndrome.
Continued monitoring, regular GCS assessments.
Empirical use of naloxone (reverses opiates), flumazenil (reverses benzodiazepines) should be considered.
Seizures should be controlled.
Supportive care – coma patients require special treatment with a multi-disciplinary approach to avoid complications such as aspiration pneumonia, pressure sores, contractures, and they will require nasogastric or parenteral feeding.
Related Topics