Chapter: Obstetrics and Gynecology: Assessment of Genetic Disorders in Obstetrics and Gynecology
Abnormalities In Chromosome Structure
ABNORMALITIES IN CHROMOSOME STRUCTURE
Structural alterations in chromosomes are less common than numerical alterations. Structural abnormalities that affect reproduction occur in 0.2% of the population.
A deletion occurs
when a portion of a chromosome seg-ment is lost (Table 7.2). In a terminal deletion, the miss-ing portion
of the chromosome is appended to the end of the long or short arm. If the
missing portion of the chro-mosome is appended to both the long and short arms
of the same chromosome, a ring
chromosome can result. An interstitial
deletion occurs when the deleted portion lacks a centromere, or in cases
involving chromosomal breakage. Insertions
occur when the portion of an inter-stitially deleted segment is inserted into a
nonhomologous chromosome.
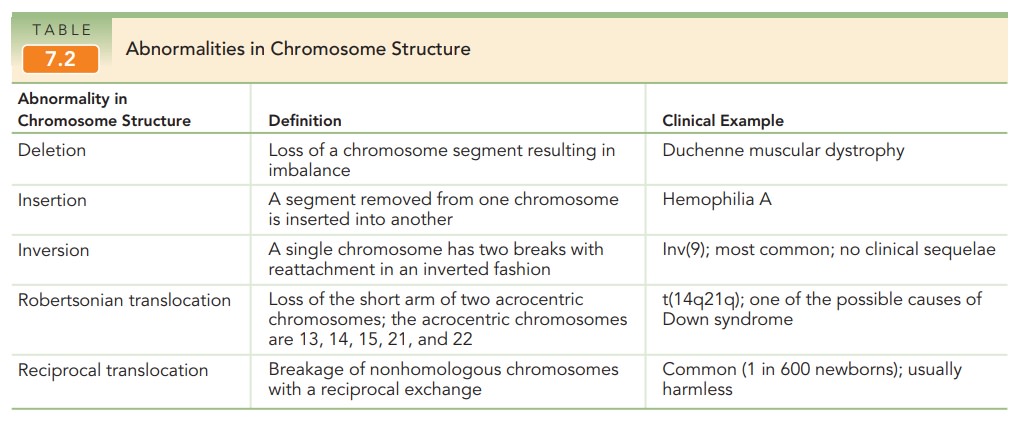
An inversion is the result of faulty repair of a chro-mosomal
breakage. The broken portion is inserted into the chromosome in an inverted
fashion. A paracentricinversion occurs
when both breaks occur on one arm ofa chromosome. These types of inversions do
not include the centromere, the
region where the chromosome pairs are joined. Paracentric inversions cannot be
iden-tified by a traditional karyotype because the arms appear to be of normal
length. Fluorescence in situ hybridization (FISH) [see p. X] with
locus-specific probes is used to detect this type of abnormality. A pericentric inver-sion involves a break
in each arm. The centromere isincluded and a notable gain or loss of genetic
material can be identified on a karyotype. For a parent with an inversion, the
risk of having an abnormal child depends on the method of detection, the
chromosome involved, and the size of the inversion. The observed risk is
approx-imately 5% to 10% if the inversion is identified after the birth of an
abnormal child, and 1% to 3% if identified at some other time. An exception is
pericentric inversion of chromosome 9, which is not associated with genetic
defects in offspring.
A translocation
involves the transfer of two chro-mosome segments,
usually between nonhomologous (non-paired) chromosomes. They are the most
common form of structural rearrangements in humans. A translocation is
described as balanced when equal
amounts of genetic material are exchanged between chromosomes, and unbal-anced when the chromosomes
receive unequal amountsof genetic material. Two types of translocations are
pos-sible. A Robertsonian translocation
only occurs in acro-centric chromosomes—those in which the centromere is
located very near one end (chromosomes 13, 14, 15, 21, and 22). A person with a
Robertsonian translocation is phenotypically normal, but the gametes they
produce may be unbalanced. Whether the unbalanced gametes will result in
abnormal offspring depends on the type of translocation, the chromosomes
involved, and the sex of the carrier parent. The most clinically important
Robertsonian translocations are those involving chromo-some 21 and another
acrocentric chromosome, most commonly chromosome 14. Carriers of these
transloca-tions are at increased risk of having a child with trisomy
The risk of trisomy 21 is 15% if
the translocation is maternal and 2% or less if it is paternal.
Balanced
reciprocal translocations may involve anychromosome and are
the result of a reciprocal exchange of chromosome material between two or more
chromosomes. Like those with Robertsonian translocations, individuals with a
balanced reciprocal translocation are also phenotyp-ically normal but may
produce gametes with unbalanced chromosomes. The observed risk for a
chromosomal abnormality in an offspring is less than the theoretical risk,
because some of these gametes result in nonviable concep-tions. In general, carriers
of chromosome translocations identified after the birth of an abnormal child
have a 5% to 30% risk of having unbalanced offspring. Children with an
unbalanced chromosome translocation are at increased risk for mental
retardation, neurodevelopmental delay, and other congenital abnormalities.
Patterns of Inheritance
Single-gene (Mendelian) disorders display predictablepatterns of inheritance related to the location of the gene (autosomal or X-linked) and the expression of the pheno-type (dominant or recessive). Although Mendelian disor-ders were the first type of genetic disorders described, it is now known that there are many genetic and environmental factors that modify these genes, making true single-gene disorders relatively rare. Health care providers should be aware that many single-gene disorders are discovered each year and may be tracked using Internet databases, such as Online Mendelian Inheritance in Man (http :/ /www.nslij-genetics .org/ search_omim. html).
Related Topics