Chapter: Essentials of Psychiatry: Social Psychology
Social Psychology: The Self
Social psychology, defined broadly as the study of
social influences on psychological functioning, is highly relevant to a
biopsychosocial perspective in that it focuses on understanding the
person–environment relationship. Environmental factors are presumed to
influence psychological functioning. Individuals are defined as active
interpreters of the environmental contexts in which they live such that
individual construals of events influ-ence psychological life and behavior.
The Self
Theory and Research Findings
Historical Precedents
Current social psychological efforts to understand
the self in the context of the person–environment relationship, particularly
the social world of the individual, are not without significant historical
precedence. For example, James (1890/1981) posited that one com-ponent of the
self was a social self determined in part by rela-tionships with significant
others. James maintained that because one’s social roles and impact on others
are varied, each individual has multiple social selves (e.g., self at work,
self with family) with varying degrees of integration and internal consistency.
Cooley’s (1902) concept of the looking-glass self referred to the idea that the
self emerges from one’s interpretations of the reactions of im-portant others
in the social environment. Similarly, Mead’s (1934) symbolic interactionism
approach posited that self-knowledge de-rives from a process of taking the role
of the other in social inter-action. According to this view, the individual
internalizes norms and expectations of the social group (the generalized other)
in the course of social interaction. This internalization of the generalized
other provides the basis for self-reflection, including the capacity to
evaluate one’s gestures and deeds, and anticipate others’ responses to one’s
behavior. Social psychological inquiries into the self in the middle decades of
the 20th century were sparse, but over the past 20 years interest in
self-functioning has dramatically increased, in part spurred by social
cognition research (Taylor, 1998). While a comprehensive review of this now
voluminous literature is beyond the scope of this discussion, a sampling of
representative, contem-porary social psychological perspectives on self is
presented here
Social Psychological Models of Self
Consistent with trends toward systematic
examination and articulation of the person–environment relationship in
personality functioning as a whole (Baumeister, 1999; Curtis, 1991; Mitchell,
2000), social psychological models presume that self-functioning is influenced
both by intrapersonal and situational context factors (Baumeister, 1998; Tesser
et al., 2000). From this perspective,
self-functioning may be understood in terms of personal traits and dispositions
(individual self), interpersonal roles and relationship patterns (relational
self), and larger group identifica-tions (collective self) (Sedikides and
Brewer, 2001).
Investigations of the self have produced myriad
conceptu-alizations of self-functioning. To organize the diverse strands of
theory and research on self, Baumeister (1998) has proposed three dimensions
central to the construction of self, including reflex-ive consciousness,
interpersonal being and executive function. Reflexive consciousness refers to
the human capacity to reflect on personal thoughts, feelings and behavior, and
is the mechanism that makes possible the construction of self-conceptions and
self-knowledge. Interpersonal being connotes the relational com-ponent of self
that develops within ongoing interpersonal trans-actions and serves the vital
psychological function of negotiating the relational world. Executive function
refers to the capacity for agency, decision-making and initiative in living,
and is the basis for active engagement with the environment. Social
psychologi-cal models of self-functioning typically presuppose and/or focus on
one or more of these dimensions of self.
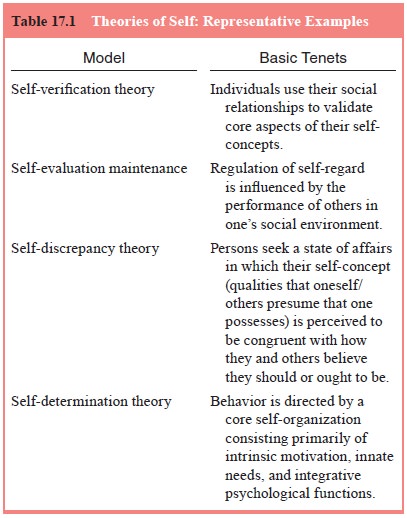
To illustrate current social psychological thinking
with regard to self-functioning, a few examples of recent social psychological
theories of self are outlined briefly in the table: the self-verification
theory, self-evaluation maintenance, self-discrepancy theory and
self-determination theory (Table 17.1). Each of these models represents a
significant contribution to the social psychological perspective on self, and
although not clinically derived, has significant relevance to the clinical
situation.
Self-presentation, Impression Management and Personal Identity
Along with specific theoretical models of self, social psychology has examined the impact of self-presentation and impression management on self-functioning. Specifically, people are invested in presenting themselves in certain ways (performing) in social situations and endeavor to control the impressions that others have of them in those situations (Goffman, 1959; Leary, 1995). These modes of self-presentation have some degree of influence on self-definition and personal identity (Tice and Baumeister, 2001). Successful impression management requires an awareness of social expectations regarding behavior in a specific situation, a desire to act within social expectations, and a capacity to present oneself in such a way that the desired impression is conveyed. One’s behavior in social interactions also is guided by the impressions one forms of others. Generally speaking, it is adaptive to be cognizant of others’ views of oneself and to portray oneself in particular ways because these interpersonal strategies can enhance one’s capacity to comprehend, regulate and anticipate social interaction patterns (Schlenker and Pontari, 2000). In deciding how to present them-selves in a social interchange, people stress the commonalities between themselves and what is expected of them and present a personally and socially desirable public image to assure social compatibility, solidarity with others and social approval.
Self in Health and Illness
Issues of physical health and illness influence
both one’s self-definition and the quality and nature of one’s interpersonal
world. In turn, one’s self-definition influences how one responds to
health-related concerns. Self-efficacy (Bandura, 1997), which connotes beliefs
regarding one’s capacity to perform a required action, is an especially
important variable in predicting individual responses to health-related
concerns (Salovey et al., 1998). To
heighten the extent to which individuals can exercise control over their own
health behaviors and associated environmental stresses, individuals may be
taught self-management and self-control tech-niques. Learning the array of
cognitive and behavioral coping strategies that increase people’s ability to
manage their illness and associated affective responses also enhances
self-efficacy and overall capacity for effective self-regulation.
Mental Health Implications
Mental health professionals increasingly have
appreciated the need to understand self-functioning in a relational context.
This shift in focus has been influenced by attachment theory (Bowlby, 1982),
interpersonal psychiatry (Sullivan, 1953), psychoanalytic object relations
theory (Greenberg and Mitchell, 1983), feminism (Jordan, 1997) and family
systems theory (Gurman and Kniskern, 1981, 1991). For example, Sullivan’s
(1953) clinical theory included a characterization of the self-system as
composed of the good-me bad-me and not-me personifications, with the
self-system defined interpersonally on the basis of perceived responses of
significant others beginning early in life. Within the psychoanalytic
tradition, adherents to object relations theory (Fairbairn, 1954; Guntrip,
1969; Winnicott, 1965), self-psychology (Kohut, 1977), and relational
psychoanalysis (Mitchell, 2000) have underscored the importance of the
interpersonal contributions to self-development and functioning. Each of these
approaches emphasizes that the nature and quality of the relationship between
the therapist and patient is centrally relevant to helping the patient make
changes in self-functioning.
Models of Self and Clinical Intervention
Based on a synthesis of theoretical models and
empirical research findings, Deaux (1992) has developed a social psychological
model of relationships between self and mental health that re-volves around
self-definition and the impact of challenges to self-definition on mental
health functioning. In the model, self-definition is conceptualized as
consisting of 1) specific domains of functioning (e.g., social and personal
identities, life tasks) rather than as a global entity; 2) goals and
aspirations as mo-tivational elements; and 3) active interpretations of
experience and personal meaning constructions. Demographic and socio-cultural
variables, social structure and socialization processes are viewed as distal
influences on self-definition. Although the self-definition is presumed to be
relatively stable, it is subject to challenge by internal factors (e.g.,
perceived discrepancies between the self-definition and internally defined
expectations for oneself, negative social comparisons) and/or external factors (e.g.,
illness, change of employment status, changes in significant relationships).
Challenge triggers a self-evaluation process to deal with information that is
inconsistent with one’s predominant self-definition. Self-evaluation results in
regulation and recon-struction activities focused internally on the self (e.g.,
self-esteem maintenance, self-affirmation, self-esteem protection, activities
associated with alterations in self-definition) and/or externally on the
external world (e.g., self-verification, self-monitoring, behavioral
disconfirmation activities associated with presen-tation of the reformulated
self-definition in the social world). Negative outcomes of the self-evaluation
process are presumed in the model to be associated with adverse mental health
outcomes.
Drawing from myriad theories and concepts from
within social psychology, Deaux’s (1992) model acknowledges the cen-trality of
self-regulation processes in the maintenance of overall mental health as
individuals respond to challenges to existing self-definitions. Self-regulation
processes are a core element of the social psychological theories of self
summarized herein, including self-verification theory (Swann, 1983, 1997),
self-evaluation main-tenance (Tesser, 1991; Beach and Tesser, 1995),
self-discrepancy theory (Higgins, 1987; Moretti and Higgins, 1999) and
self-de-termination theory (Deci and Ryan, 2000; Ryan and Deci, 2000). Each of
these models provides insights for the clinical under-standing and treatment of
mental health problems as they relate to challenges to self-definition and the
self-evaluation processes that ensue in response to such challenges. Examples
of the clini-cal relevance and utility of these models for clinical work now
will be considered.
Self-presentation and Impression Management in Clinical Perspective
While the maintenance of a specific social image
through impression management can yield psychological benefit, certain patterns
of self-presentation can also have a negative psychological impact. For
example, preoccupation with presenting oneself as competent in a particular
pursuit when realistic appraisal sug-gests otherwise can give rise to pursuit
of goals for which one is not suited, generating impractical expectations for
self and precipitating associated frustration and disappointment. Extreme
efforts to present oneself in a particular light can lead to maladap-tive
states of mind, response patterns and relationships (Shepperd and Kwavnick,
1999).
Impression management also has implications for the
self-relevant social emotions of guilt and shame. Both guilt and shame are
responses to perceived transgressions on the part of the self, but differ in
that guilt involves condemnation of a particular behavior and is accompanied by
remorse or regret, whereas shame involves condemnation of one’s self and is
ac-companied by feelings of being exposed as objectionable and bad (Tangney and
Salovey, 1999). Both guilt and shame are emotional experiences tied to one’s
perceived failure to maintain a positive self-presentation, and each propels
specific patterns of impres-sion management. For instance, guilt tends to spark
interpersonal efforts to make reparation for one’s behavior, whereas shame may
prompt social avoidance associated with a wish to hide the self from view
(Tangney and Salovey, 1999). Although guilt and shame are expectable emotional
dimensions of everyday psycho-logical life, their problematic manifestations
can adversely affect both self-regulation and interpersonal relationships, and
there-fore must be considered in clinical evaluation and treatment of
psychological dysfunction.
Related Topics