Chapter: Basic Radiology : Liver, Biliary Tract, and Pancreas
Exercise: Upper Abdominal Trauma
EXERCISE 11-3.
UPPER ABDOMINAL TRAUMA
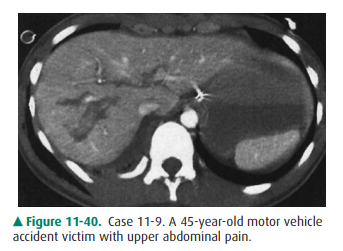
11-9. What is the most likely diagnosis in Case 11-9 (Figure
11-40)?
A.
Hepatic contusion
B.
Hepatic laceration
C.
Uncomplicated ascites
D.
Hemoperitoneum
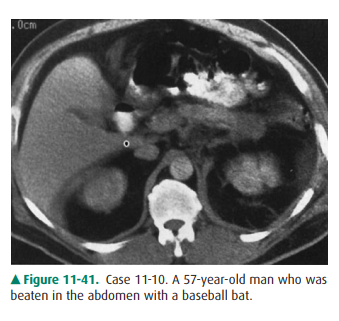
11-10. What is the most likely diagnosis in Case 11-10 (Figure
11-41)?
A.
Pancreatic trauma
B.
Bowel injury
C.
Mesenteric injury
D.
Hepatic laceration
Radiographic Findings
11-9. In this case, the liver has an irregularly linear lesion
in its central aspect, representing a liver laceration (B is the correct answer
to Question 11-9).
11-10. In this case, there is a low-density bulbous enlarge-ment
of the pancreatic tail, representing a pancreatic injury (A is the correct
answer to Question 11-10).
Discussion
Hepatic injury is common after
blunt trauma. Hepatic in-juries may be life-threatening as a result of bleeding
and shock, but more often surgery is not required. Observation and systemic
support may be the only treatment necessary. Like trauma to any other organ,
injury to the liver varies from mild to severe. A mild injury of the liver
produces a localized collection of traumatized liver tissue and an interstitial
hematoma, like a bruise, which is termed a contusion.
More severe injuries that involve
complete disruption of the tissue into fracture planes, perhaps involving the
hepatic veins, inferior vena cava, or portal veins, are called lacerations.
Most blunt abdominal trauma in
the United States is radi-ographically evaluated with CT. Angiography is used
to a lesser extent. US, NM, and MR imaging are of little or no value in a
general survey of abdominal trauma. On CT, hepatic contusion is seen as a
low-attenuation lesion, perhaps with mass effect on surrounding hepatic
vessels. Associated hemoperitoneum is not usually seen. On CT, hepatic
laceration appears as an irreg-ular, stellate, or linear lesion through the
liver parenchyma (Figure 11-40), sometimes extending to the porta hepatis,
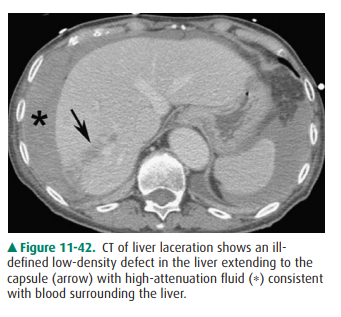
liver capsule, or IVC (Figure 11-42). A hallmark of severe trauma to upper abdominal
organs is accompanying hemoperitoneum, which appears as a collection of
high-density material at the site of bleeding and is termed the sentinel clot.
Acute blood that has migrated away from the site of active bleeding, or old
hemoperitoneum at any site, often has the attenuation of sim-ple or near-simple
fluid and can resemble intraperitoneal fluid, or ascites, from a number of
causes. NM hepatobiliary scans, also called HIDA (hepatobiliary iminodiacetic
acid) scans, can be used to assess for a bile leak if that is suspected.
Ascites is a nonspecific reaction
of the peritoneal space to a variety of causes, including tumor, inflammation,
trauma, increased systemic venous resistance (eg, congestive heart failure),
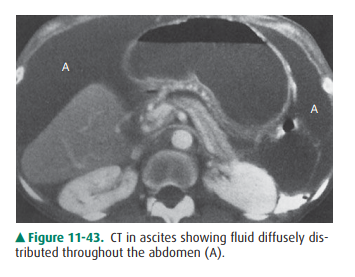
renal or hepatic insufficiency, and many other con-ditions. It is characterized
by the production of intraperi-toneal fluid. This fluid can be simple, a
transudate, in which case it has fluid density (Figure 11-43) and is free to
move tothe dependent portion of the abdominal or pelvic cavity with patient
movement. Alternatively, it can be complex, an exudate, in which case it is
denser than simple fluid, is ac-companied by solid tissue (eg, tumor deposits
in peritoneal metastases) or layered material (eg, blood from trauma or
inflammatory cellular debris in peritonitis), and often is loc-ulated, or
unable to move freely throughout the intraperi-toneal cavity (eg, abscess).
Pancreatic injury is uncommon,
but potentially serious. Mortality from pancreatic injuries is nearly 20%.
Being crushed against the spine probably accounts for the fre-quency of injury
to the body of the pancreas. Pancreatic trauma may or may not be associated
with increased amylase. Usually caused by blunt trauma, pancreatic trauma is
often associated with injuries to other organs, such as liver and bowel. These
injuries produce intraperitoneal blood and fluid and interstitial mesenteric
edema, which can be confus-ing. As with hepatic trauma, CT with intravenous
contrast is usually the modality of choice to evaluate pancreatic trauma, but
even on CT, the diagnosis can be difficult. On CT, the pancreas may be ill
defined, enlarged, or even disrupted, that is, fractured.
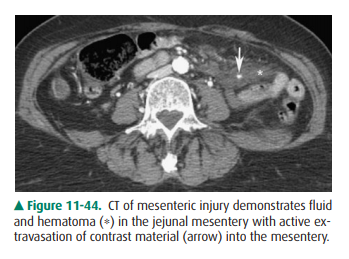
Bowel and mesenteric injuries are
found in approxi-mately 5% of all patients undergoing laparotomy after motor
vehicle accidents. Injuries of the bowel and mesen-tery frequently accompany
injury to the liver or pancreas. These injuries can result in massive
intraperitoneal bleed-ing from disruption of mesenteric vessels, or peritonitis
from bowel perforation. As elsewhere, CT is the modality of choice to evaluate
patients for possible bowel or mesenteric injuries, but these injuries, like
those to the pancreas, can be difficult to detect. On CT, injuries of the bowel
and mesen-tery include free air with the intraperitoneal or retroperi-toneal
spaces, free intra-abdominal fluid, circumferential or eccentric bowel wall
thickening, enhancement of the bowel wall, streaky soft-tissue infiltration of
the mesenteric fat, free mesenteric hematoma (Figure 11-44), and especiallysentinel
clot. Angiography may demonstrate free extravasa-tion of contrast material in
injuries of the mesenteric ves-sels, and percutaneous embolization may stop
bleeding when surgery is not possible.
Related Topics