Chapter: Basic Radiology : Gastrointestinal Tract
Exercise : Colonic Bleeding
EXERCISE 10-5.
COLONIC BLEEDING
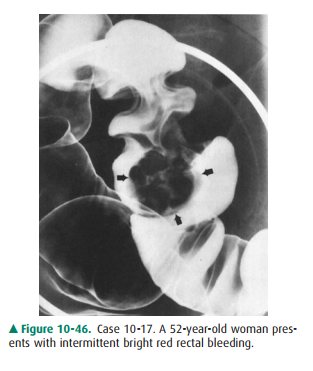
10-17. What is the most likely cause of the large polypoid
le-sion (arrows) in the sigmoid colon in Case 10-17 (Figure 10-46)?
A.
Annular carcinoma
B.
Benign lipoma
C.
Polypoid carcinoma
D.
Pedunculated benign adenoma
E.
Hyperplastic polyp
10-18. What is the etiology of the irregular, focal narrowing in
the ascending colon in Case 10-18 (Figure 10-47)?

A.
Polypoid carcinoma
B.
Annular carcinoma
C.
Inflammatory stricture
D.
Surgical anastomosis
E.
Ischemic stricture
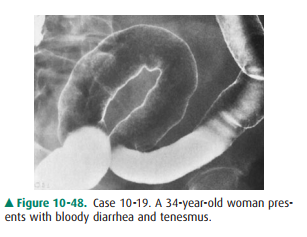
10-19. What is the most likely
explanation of the diffuse rec-tosigmoid mucosal abnormality on double-contrastbarium
enema in Case 10-19 (Figure 10-48)?
A.
Ischemic colitis
B.
Pseudomembranous colitis
C.
Lymphogranuloma venereum
D.
Crohn colitis
E.
Ulcerative colitis
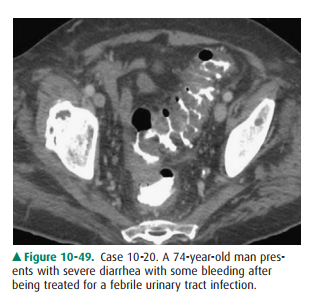
10-20 What is the least
likely cause of the diffuse wall thick-ening of the sigmoid colon seen on the
CT image inCase 10-20 (Figure 10-49)?
A.
Annular carcinoma
B.
Pseudomembranous colitis
C.
Diverticular disease
D.
Crohn colitis
E.
Radiation rectosigmoiditis
Radiologic Findings
10-17. The large, lobulated (ie, irregular surface) polypoid
mass in the sigmoid colon was a polypoid carcinoma (C is the correct answer to
Question 10-17).
10-18. The circumferential, irregular narrowing of the
as-cending colon was an annular carcinoma (B is the correct answer to Question
10-18).
10-19. The diffuse and continuous mucosal granularity seen in
the rectosigmoid colon is most consistentwith ulcerative colitis (E is the
correct answer to Question 10-19).
10-20. The diffuse wall thickening of the sigmoid colon likely
is due to an inflammatory (colitis) disorder or diverticular disease; a
pseudomembranous colitis was the cause in this patient (A is the correct answer
to Question 10-20).
Discussion
Rectal bleeding can result from a
multitude of abnormalities throughout the gastrointestinal tract. In this
exercise, the more important colonic cause of rectal bleeding are illus-trated.
Another common cause of rectal bleeding is divertic-ular disease of the colon,
which is readily shown on barium enema and CT examination. In older patients,
ischemic coli-tis and vascular malformations (eg, angiodysplasia) of the right
side of the colon are increasingly important causes. In general, contrast
studies of the gastrointestinal tract can de-tect many abnormalities that may
be a source of bleeding but cannot determine whether the lesion is bleeding
actively; cross-sectional imaging (with and without vascular contrast
material), nuclear medicine, and angiography can demon-strate active bleeding,
which can also be treated by interven-tional radiology or endoscopy.

The two most common polypoid
lesions of the colon are the hyperplastic and neoplastic polyp. Most
hyperplastic polyps are less than 5 mm in diameter, are sessile and smooth, and
may resemble small neoplastic polyps of similar size. Neoplastic polyps have a
broad pathologic spectrum, which includes: (1) benign adenomas (tubular,
tubulovillous, and villous types); (2) adenomas with focal carcinoma;
andpolypoid carcinoma. Consequently, the radiologic ap-pearances of neoplastic
colonic polyps are varied, and benign and malignant neoplasms may appear
similar. Neoplastic polyps can be sessile or pedunculated and smooth or
lobu-lated (Figure 10-50). Size is an important radiologic criterion to
estimate the risk of malignancy in a sessile colonic polyp; a polyp less than 1
cm in size has only a 1% chance of malig-nancy, with the risk increasing to 10%
for 1- to 2-cm polyps and 25% or more for polyps over 2 cm. The finding of a
pedi-cle is important because invasion of a cancer, if present, to the adjacent
colonic wall is rare. Imaging of the large bowel for colon cancer screening has
changed in recent years, with the barium enema assuming a minor role;
colonoscopy is now most often performed both for detection of neoplastic le-sions
and for their removal, which is possible in most pa-tients. CT colonography may
become more important as a screening modality, but its efficacy is under
intense investiga-tion presently.
Adenocarcinoma of the colon is
the second most com-mon malignancy that affects both sexes. About 95% of
colonic carcinomas occur in patients older than 40 years, with a peak in the
later seventh decade. As with adenocarci-nomas elsewhere in the
gastrointestinal tract, a variety of morphologic forms are seen, including
polypoid carcinoma (malignant potential discussed previously), ulcerative andinfiltrative
types, and the annular carcinoma; the last is also called the “apple-core”
lesion. In the colon of an adult pa-tient, an irregular constricting lesion
having an abrupt tran-sition with the normal colonic wall is nearly always an
adenocarcinoma (Figure 10-51). Inflammatory strictures and surgical anastomosis
typically have a smooth and often tapered appearance.

Ulcerative and Crohn colitis are
the two common idio-pathic inflammatory diseases of the colon. Other causes of
colitis include infections of various types, drug-related types (ie,
pseudomembranous colitis), radiation-induced colitis (usually proctitis),
ischemic colitis, and miscella-neous disorders. These other disorders may mimic
idio-pathic colitis, and clinical correlation and exclusion of infection are
important. Radiographic differentiation be-tween ulcerative and Crohn colitis
is usually possible in most patients; of course, cross-sectional imaging, endoscopy,
and pathologic evaluation have important roles. The features most suggestive of
ulcerative colitis are continuous disease with rectal involvement, ahaustral
shortening of the colon, and a finely ulcerated or granular mucosal surface.
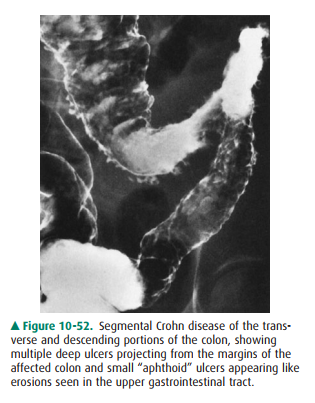
The morespecific findings of Crohn colitis include discontinuous dis-ease (ie,
skip areas) with ileitis, eccentric wall involvement, discrete (ie, aphthoid
ulcers) or deep ulceration, intramural fissuring, and formation of fistula to
adjacent organs (Figure 10-52). Complications that may occur in idiopathic
colitis include toxic megacolon, carcinoma, sclerosing cholangitis, and
abnormalities of the eyes, skin, and joints. Toxic megacolon and complicating
carcinoma are more common in ulcerative colitis.
Pseudomembranous colitis has
emerged as a common in-flammatory condition of the large bowel in recent
decades, especially in hospitalized patients. Although a number of risk factors
have been identified, the vast majority of cases are as-sociated with
antibiotic exposure. These drugs alter the intes-tinal flora, resulting in an
overgrowth of Clostridium difficile,
which releases a toxin(s) that produces the inflammatory pseudomembranes and
other pathologic changes. Imaging findings, often best seen on CT examination,
include wall thickening that may be segmental or pancolonic, fold thick-ening
causing an “accordion sign,” and mucosal irregularity due to the
pseudomembranous changes; these abnormalities are often nonspecific, and other
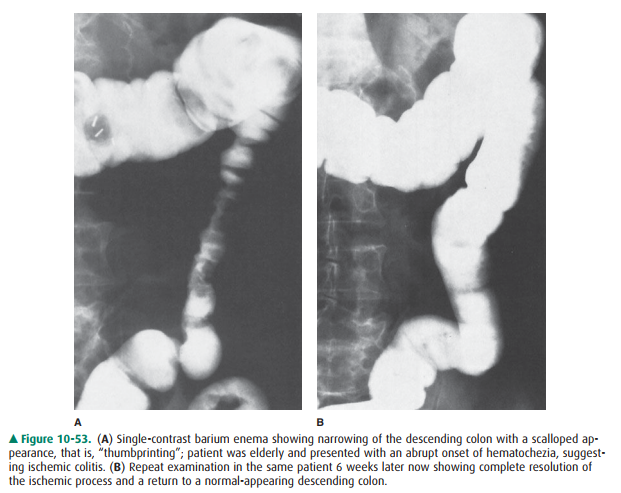
diagnostic tests (eg, sigmoi-doscopy) need to be performed. Ischemic colitis is
common in older patients and warrants further discussion. As in the small
bowel, a variety of vascular changes may cause colonic ischemia. The most
common site of involvement is in the watershed area of the main mesenteric
vessels, that is, the splenic flexure and descending colon, although other
areas and diffuse involvement of the colon may be seen. In the severest form,
colonic infarction and perforation may occur; however, the most common
appearances relate to submu-cosal hemorrhage, which causes narrowing of the
affected colon associated with irregular, smooth margins often called
“thumbprinting”; complete healing and return to normal may occur (Figure
10-53), or progression to a smooth, ta-pered stricture can result.
Related Topics