Chapter: Essential Anesthesia From Science to Practice : Clinical management : Vascular access and fluid management
Blood loss - Fluid management
Blood loss
When we
anticipate a large blood loss, we might calculate the “allowable blood loss”
(ABL) – not the amount we “allow” the surgeon to lose, but rather the volume at
which we would likely need to transfuse.
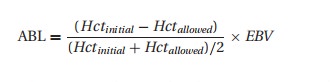
where we
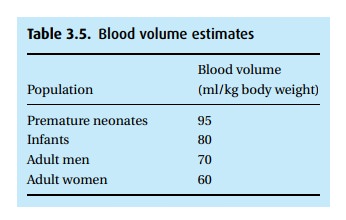
use the initial and minimum acceptable hematocrits, and the estimated blood
volume (Table 3.5). Unfortunately, we
struggle to determine when we have reached the ABL. We report the estimated
blood loss by looking at the surgical field, checking the volume in the suction
canisters (subtracting any irrigation used), and examining the surgical sponges
(a soaked 4×4 holds about 15 mL blood, a soaked lap sponge,
150 mL). More accurate, but generally impractical measures include weighing the
sponges or washing them out and checking the color of the effluent. In lieu of an accurate measure, we use
hemodynamic clues as well as serial hemoglobin concentrations.
This
brings up the common misconception that we can assess blood loss by checking
the hematocrit or hemoglobin concentration. Unless the patient has been
carefully hydrated back to “euvolemia” (normal total blood volume), this is not true! Only if an equal volume of
some other fluid is added (either from the interstitial space, or by us) does
the hematocrit fall. If left to nature’s device, it may take up to 2 days to
reach steady state. Depending on the fluid, often much more than the actual
blood loss must be given to account for the small percentage that actually remains
intravascularly. The volume that escapes is not lost though; it replenishes the
interstitial space that so generously donated fluid to the blood stream before
treatment could be instituted. This replenishment is vital for the transport of
oxygen between the blood and tissues. Massive hemorrhage and hypotension
compromise oxygen delivery to tissues; to maintain cellular integrity, these
cells resort to anaerobic metabolism, with a by-product of lactic acid. We
often gauge our resuscitation by the severity of the lactic acidosis.
Related Topics