Chapter: Ophthalmology: Eye Optics and Refractive Errors
Astigmatism
Astigmatism
Definition
Astigmatism is derived from the Greek word
stigma (point) and literally means lack of a focal point. The disorder is
characterized by a curvature anomaly of the refractive media such that parallel
incident light rays do not converge at a point but are drawn apart to form a
line.
Epidemiology:
Forty-two per cent of all humans have astigmatism greaterthan or
equal to 0.5 diopters. In approximately 20%, this astigmatism is greater than 1
diopter and requires optical correction.
Pathophysiology:
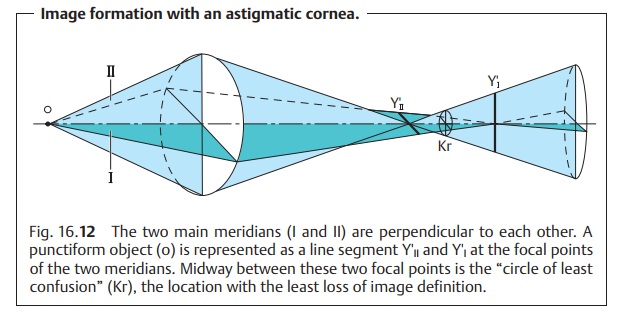
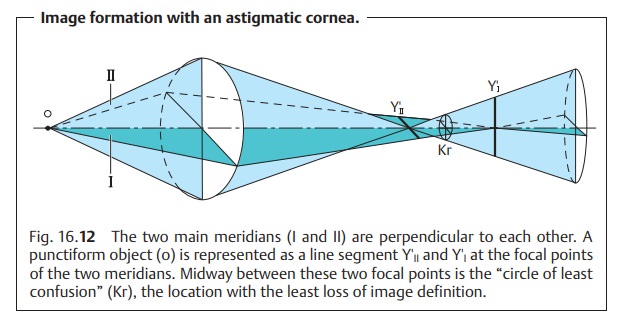
The refractive media of the astigmatic eye are not spheri-cal
but refract differently along one
meridian than along the meridian perpen-dicular to it (Fig. 16.12). This produces two focal points.
Therefore, a punc-tiform object is
represented as a sharply defined line segment
at the focal pointof the first meridian but also appears as a sharply
defined line segment rotated 90 degrees at the focal point of the second
meridian. Midway between these two focal points is what is known as the “circle of least confu-sion.” This refers
to the location at which the image is equally distorted inevery direction,
i.e., the location with the least loss of image definition.
The aggregate system lacks a focal point.
The combined astigmatic components of all of
the refractive media com-prise the total astigmatism of the eye. These media include:
❖Anterior surface of the cornea.
❖ Posterior surface of the cornea.
❖Anterior surface of the lens.
❖ Posterior surface of the lens.
Rarely, nonspherical curvature of the retina
may also contribute to astig-matism.
Classification and causes:
Astigmatism can be classified as follows:
❖ External astigmatism: astigmatism of the anterior surface of the cornea.
❖Internal astigmatism: the sum of the astigmatic components of the other media.
Astigmatism can also be classified according to the location of the meridian
ofgreater refraction:
❖ With-the-rule astigmatism (most common form): The meridian with thegreater refractive
power is vertical, i.e., between 70 and 110 degrees.
❖ Against-the-rule astigmatism: The meridian with the greater refractivepower is horizontal,
i.e., between 160 and 20 degrees.
❖ Oblique astigmatism: The meridian with the greater refractive power isoblique, i.e.,
between 20 and 70 degrees or between 110 and 160 degrees.
The discussion up to this point has proceeded
from the assumption that the anomaly is a regular astigmatism involving only two meridians approxi-mately
perpendicular to each other (Fig. 16.12). This is presumably caused by excessive
eyelid tension that leads to astigmatic changes in the surface of the cornea.
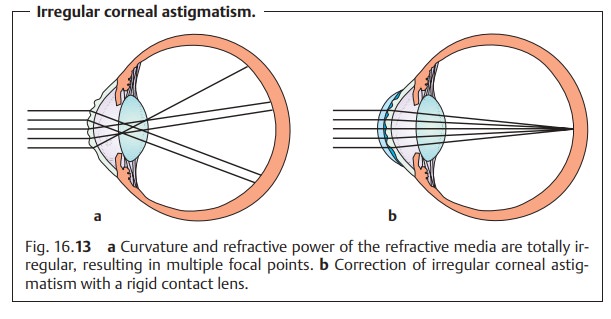
The condition above should be distinguished
from irregular astigmatism. Here, the curvature and the refractive power of the refractive
media are completely irregular (Fig.
16.13a). There are multiple focal points, which pro-duces a completely
blurred image on the retina. This condition may be caused by the following
diseases:
❖Corneal ulcerations with resulting scarring of
the cornea.
❖ Penetrating corneal trauma.
❖ Advanced keratoconus.
❖ Cataract.
❖ Lenticonus.
Symptoms:
Patients with astigmatism see everything distorted. Attempts
tocompensate for the refractive error by accommodation can lead to asthenopic
symptoms such as a burning sensation in the eyes or headache.
Diagnostic considerations:
The keratoscope(Placido
disk) permitsgrossestimation of
astigmatism. The examiner evaluates the mirror images of therings on the
patient’s cornea. In regular astigmatism,
the rings are oval; in irregular astigmatism, they are irregularly distorted. Computerized
cornealtopography (videokeratoscopy)
can be used to obtain an image of the dis-tribution of refractive values over
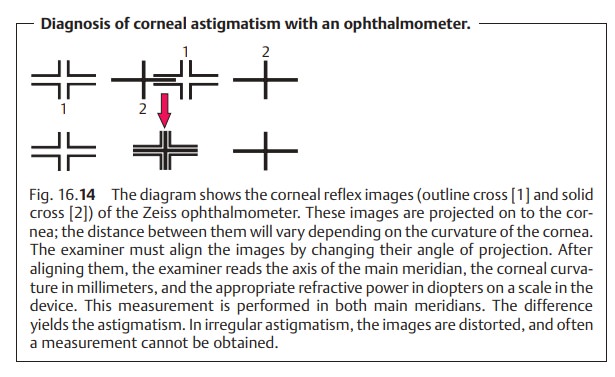
the entire cornea (see Fig. 5.3). A Helmholtzor Javal ophthalmometer can be
used tomeasure the central corneal
curva-ture, which determines the refractive power of the cornea (Fig. 16.14).
Treatment:
Early correction is crucial. Untreated astigmatism in children
willeventually lead to uncorrectable refractive amblyopia because a sharp image
is not projected on the retina.
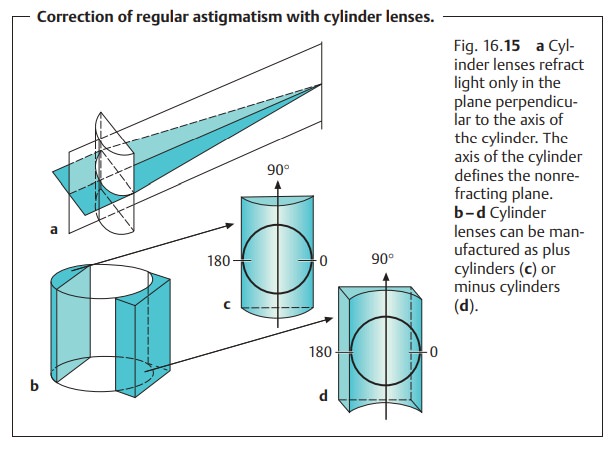
Treatment of regular astigmatism: The purpose of the correction is to bringthe “focal lines” of two main meridians together at one focal point. This requires a lens that refracts in only one plane. Cylinder lenses are required for this application (Fig. 16.15a). Once the two “focal lines” have been converged into a focal point, additional spherical lenses can be used to shift this focal point on to the retina if necessary.
Treatment of irregular astigmatism: This formcannotbe
corrected with eye-glasses. External
astigmatism may be managed with a rigid contact lens (Fig. 16.13b), keratoplasty, or surgical
correction of the refractive error. Irregular internal astigmatism is usually lens-related. In this case, removal
of the lens with implantation of an intraocular lens is indicated.
Only regular astigmatism can be corrected with
eyeglasses.
Related Topics