Chapter: Obstetrics and Gynecology: Cancer of the Uterine Corpus
Uterine Sarcoma
UTERINE SARCOMA
Uterine
sarcomas represent an unusual gynecologic malignancy accounting for
approximately 3% of cancers involving the body of the uterus, and only about
0.1% of all myomas. Progressiveuterine enlargement
occurring in the postmenopausal years should not be assumed to be the result of
simple uterine leiomyomata, because appreciable endogenous ovarian estrogen
secretion is absent, thereby minimizing the poten-tial for growth of benign
myomas. Even postmenopausal women on low-dose hormone therapy are not at risk
for stimulation of uterine enlargement. When progressive growth is present in
postmenopausal women, uterine sar-coma should be considered. Other symptoms of
uterine sarcoma include postmenopausal bleeding, unusual pelvic pain coupled
with uterine enlargement, and an increase in unusual vaginal discharge.
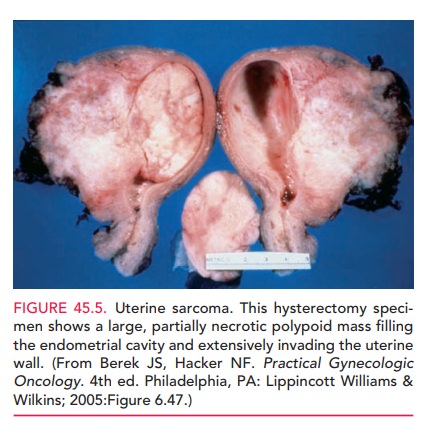
Surgical removal is the method of most reliable diagnosis. Accordingly,
hysterectomy is usu-ally indicated in patients with documented, and especially
progressive, uterine enlargement (Fig. 45-5).
The virulence of uterine sarcoma
is directly related to the number of mitotic figures and degree of cellular
atypia as defined histologically. These tumors are more likely to spread
hematogenously than endometrial adenocarci-noma. When uterine sarcoma is
suspected, patients should undergo a tumor survey to assess for distant
metastatic dis-ease. At the time of hysterectomy, it is necessary to
thor-oughly explore the abdomen and sample commonly affected node chains,
including the iliac and periaortic areas. Thestaging
for uterine sarcoma is surgical and identical to that for endometrial
adenocarcinoma.
Unfortunately, the 5-year
survival of patients with a uterine sarcoma is only 50%. Radiation and
chemotherapy provide little benefit as adjuvant therapy to hysterectomy.
Related Topics