Chapter: Medical Surgical Nursing: Assessment of Renal and Urinary Tract Function
Urinalysis and Urine Culture - Diagnostic Evaluation
Diagnostic Evaluation
URINALYSIS
AND URINE CULTURE
The
urinalysis provides important clinical information on kidney function and helps
diagnose other diseases, such as diabetes. The urine culture determines if
bacteria are present in the urine, as well as their strains and concentration.
Urine culture and sensi-tivity also identify the antimicrobial therapy that is
best suited for the particular strains identified, taking into consideration
the an-tibiotics that have the best rate of resolution in that particular
geo-graphic region. Appropriate evaluation of any abnormality can assist in
detecting serious underlying diseases.
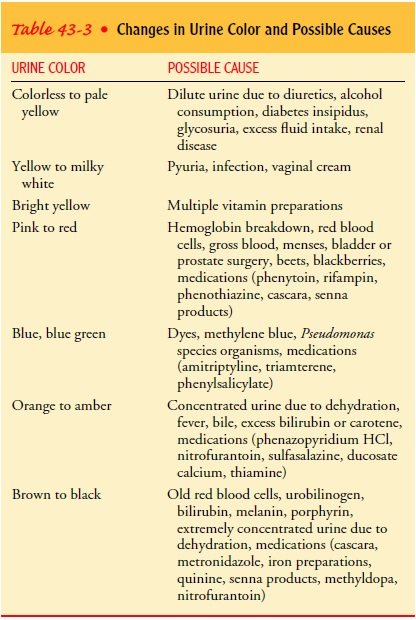
Urine
examination includes the following:
· Urine color (Table 43-3)
· Urine clarity and odor
· Urine pH and specific
gravity
· Tests to detect protein,
glucose, and ketone bodies in the urine (proteinuria, glycosuria, and
ketonuria, respectively)
· Microscopic examination
of the urine sediment after cen-trifuging to detect RBCs (hematuria), white blood cells, casts (cylindruria), crystals
(crystalluria), pus (pyuria), and
bacteria (bacteriuria)
Significance of Findings
Several abnormalities, such as hematuria and proteinuria, pro-duce no symptoms but may be detected during a routine urinal-ysis using a dipstick. Normally, about 1 million RBCs pass into the urine daily, which is equivalent to one to three RBCs per high-power field. Hematuria (more than three RBCs per high-power field) can develop from an abnormality anywhere along the genitourinary tract. Common causes include acute infection (cys-titis, urethritis, or prostatitis), renal calculi, and neoplasm. Other causes include systemic disorders, such as bleeding disorders; ma-lignant lesions; and medications, such as warfarin (Coumadin) and heparin. Although hematuria may initially be detected using a dipstick test, further microscopic evaluation is necessary (Na-tional Institute of Diabetes & Digestive & Kidney Diseases [NIDDK], 1999).
Protein
in the urine (proteinuria) may be a benign finding, or it may signify serious
disease. Occasional loss of up to 150 mg/day of protein in the urine, primarily
albumin and Tamm-Horsfall protein, is considered normal and usually does not
require further evaluation. A dipstick examination, which can detect from 30 to
1,000 mg/dL of protein, should be used as a screening test only, because urine
concentration, pH, hematuria, and radiocontrast materials all affect the
results. Because dipstick analysis does not detect protein concentrations of
less than 30 mg/dL, the test can-not be used for early detection of diabetic
nephropathy. Micro-albuminuria (excretion of 20 to 200 mg/dL of protein in the
urine) is an early sign of diabetic nephropathy. Common benign causes of
transient proteinuria are fever, strenuous exercise, and prolonged standing.
Causes
of persistent proteinuria include glomerular diseases, malignancies, collagen
diseases, diabetes mellitus, preeclampsia, hypothyroidism, heart failure,
exposure to heavy metals, and use of medications, such as nonsteroidal
anti-inflammatory drugs (NSAIDs) and angiotensin-converting enzyme inhibitors
(NIDDK, 2000).
Related Topics