Chapter: Biochemical Pharmacology : Introduction
Strategies of drug development
Strategies of drug
development
Drug development strategies
may be classified as follows:
1. Rational design
2. Brute force
3. Traditional medicine / natural products
4. Mere chance.
Note that these distinctions
are not really sharp in practice. E.g., the development of H2-receptor
blockers described above would be a mixture of strategies 1 and 2. In reality,
one will always try to rationally make use of as much infor-mation as possible
and then play some kind of lottery to do the rest.
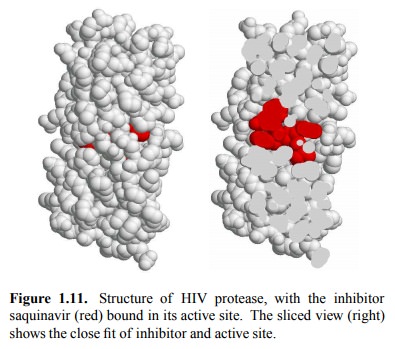
An example of the rational
approach to drug design is pro-vided by the development of HIV (human immune
defi-ciency virus) protease inhibitors. HIV protease cleaves vi-ral
polyproteins – the initial products of translation – into the individual
protein components and thus is essential for the maturation of virus particles.
The crystal structure of HIV protease was used to design synthetic molecules
that would snugly fit into the active site. Figure 1.11 shows the inhibitor
saquinavir bound to the the enzyme. HIV pro-tease inhibitors have become one of
the mainstays of HIV therapy; their use in combination with reverse
transcrip-tase inhibitors greatly extends the life expectancy of HIV patients.
The brute-force approach
involves the following steps:
1. Systematically test every new (or old) compound
for drug activity in all kinds of drug activity assays – no matter which
purpose it was designed for
2. If you stumble upon something, figure out how
it works
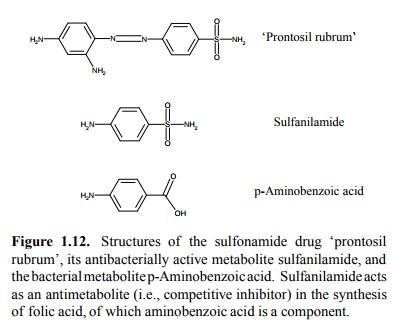
A classic success case of the
brute-force approach is the discovery of `Prontosil rubrum', the first
sulfonamide type antibacterial drug (Figure 1.12). `Rubrum' means `red' in
Latin – so this is another dye turned drug. The biochemical mechanism was
completely unknown by the time, but the drug nevertheless was very active
against a considerable range of bacterial species. The discovery of
sulfonamides in the 1930s was a major reason for the delay in the devel-opment
of penicillin, the effect of which was discovered in 1928 but which was not
available for clinical use before 1942 (see below).
The brute force approach to
drug discovery is still widely used, and one of the reasons why drug design is
now large-ly done by major pharmaceutical companies. In fact, pron-tosil was
discovered at the biggest pharmaceutical compa-ny of the era, the German `IG
Farben', which was disman-tled after the war for its involvement with the
production of poisons used in the holocaust.
Traditional medicine is
largely based on plants and their various poisons. There is a fair number of
drugs original-ly isolated from plants that are still being used in clinical
medicine – even if most of them are now prepared synthet-ically. This approach
may be summarized as follows:
1. Isolate the active components from
therapeutically useful and / or toxic plants
2. Elucidate structure, mode of action
3. Find synthetic route, create novel derivatives
with im-proved properties
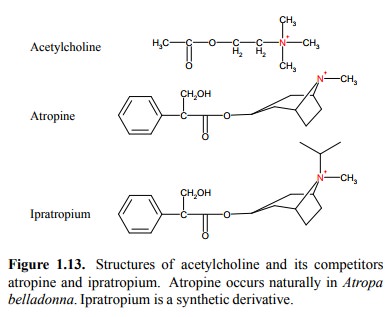
A classical example is
atropine (Figure 1.13). It is isolated from the plant Atropa belladonna. `Bella donna' is a com-mon phrase in schmaltzy
songs of (true or pretended) Ital-ian origin and means `beautiful woman'. In
the old days, atropine was used by young women to augment their looks before
attending festivities. It widens the pupils of the eyes, and it prevents
sweating, therefore leading to accumulation of heat and to red cheeks. At
higher dosages, it also caus es hallucinations, which may or may not be
helpful with falling in love. The hallucinations are, obviously, caused by
atropine entering the central nervous system.
The central effects are lessened by derivatization of the tertiary amine
found in atropine to a quaternary amine, as in ipratropium. Because of its
permanent charge, ipratropium does not easily cross the blood brain barrier by
`non-ionic diffusion', and it is therefore often preferred over atropine in
clinical medicine.
The final approach to drug
development consists in taking advantage of
mere chance. The most striking example that comes to mind is the
discovery of penicillin. Here is a summary of this `strategy':
1. Forget to properly cover your petri dish and
2. Have the petri dish contaminated by a mold
that kills bacteria (Sir Alexander Fleming, 1929),
3. Wait until somebody else purifies the active
ingredient and makes it available for clinical use (Florey and Chain, 1942).
S.A.Waksman took up this
paradigm of drug discovery in the 1940's
in a more systematic way, starting at stage 2 rather than 1. He succeeded in
isolating a large number of antibiotics from a wide variety of soil
microorganisms, particularly streptomycetes. The first example was thyrotricin,
which is useful for local treatment only.
More prominent discoveries of his are streptomycin and chloramphenicol,
which can be used systemically and still have their place in therapy today.
Related Topics