Chapter: Surgical Pathology Dissection : The Urinary Tract and Male Genital System
Penis : Surgical Pathology Dissection
Penis
Foreskin
Foreskins
removed from infants are usually not submitted to the surgical pathology
laboratory for examination. If you do receive one of these specimens, measure
it, describe its appearance, and submit a section for histologic evaluation.
Foreskins removed from older patients are rou-tinely submitted for evaluation,
because they are more likely to harbor pathology. You need to sample these
specimens more extensively and pay close attention to the margin of resection.
Ink the epithelial margin, and carefully inspect the surfaces of the specimen.
Record the number, size, location, and appearance of any lesions. Because the
foreskin is much easier to section once it is fixed, you may wish to pin the
four corners of the foreskin onto a wax tablet, and submerge the specimen in
formalin.
Even if
no lesions are appreciated on gross inspection, liberally sample foreskins
removed from adults to look for early neoplastic changes. Use perpendicular
sections so that the epithelial margin is included in the sections. When a
neo-plasm is suspected, each quadrant of the epithe-lial margin should be
sampled. More extensive sampling may be necessary if a visible lesion is large
or if the lesion approaches the margin at several sites.
Penectomies
The
diverse findings encountered in penectomies range from the essentially normal
penis removed from a patient undergoing a sex change operation to the penis
grossly distorted by gangrene orinfiltrating carcinoma. The best way to be
pre-pared for virtually any penectomy specimen is to become familiar with the
anatomy of the normal penis. This familiarity will allow you to answer those
questions that should be foremost in mind when evaluating a penile lesion:
Where on the penis does the lesion arise, into what anatomic compartments does
the lesion extend, and how close is it to the resection margin?
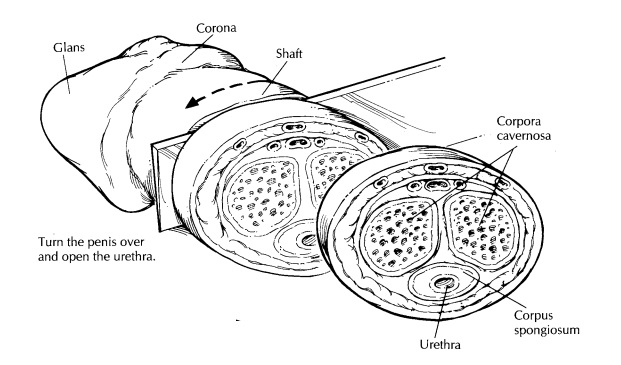
Before
beginning the dissection, identify the three basic structural components of the
penis as illustrated. The shaft, as
its name suggests, is the cylindrical rod-like portion of the penis. It is
cov-ered by a loosely attached layer of rugated skin, and it houses the three
erectile bodies of the penis—the two corpora cavernosa (located dor-sally and
laterally) and the single corpus spongio-sum (located ventrally, surrounding
the urethra along the midline). The glans
is the cone-shaped expansion of the distal corpus spongiosum. It sits like a
bonnet on the end of the shaft. The edge of the glans at its base is referred
to as the corona, and at the apex of the glans is the opening of the urethra
(i.e., the urethral meatus). The foreskin
is a retractable fold of skin that partially covers the glans. Its attachment
to the skin of the shaft occurs just behind the corona. The foreskin will
obviously not be present in penectomies from circumcised males.
Carefully
examine the surfaces of the specimen, keeping in mind that the vast majority of
penile neoplasms arise from the surface epithelium of the glans and from the
undersurface of the foreskin. Neoplasms may be concealed by the foreskin, so be
sure to retract this skin fold and look at the entire surface including the
epithelium lining the deep recesses of the coronal sulcus. Other
neoplasms—especially those that are notdeeply invasive—may be so subtle as to
elude casual inspection; therefore, be sure to look carefully for discolored
plaque-like irregularities that characterize superficial spreading carcino-mas.
Do not stop once one lesion has been found; keep looking for others. Squamous
carcinomas of the penis tend to be multifocal, and these tumors will be
overlooked if the entire epithelial surface is not examined.
In the
gross description, record the dimensions of the entire specimen and the
dimensions of each of its individual components (i.e., foreskin, glans, and
shaft). Describe the surfaces of each component, and note the number, size,
color, and distribution of any lesions found. Assess the tumor’s macroscopic
pattern of growth (e.g., nod-ular, ulcerative/infiltrative, verrucous, or
flat).
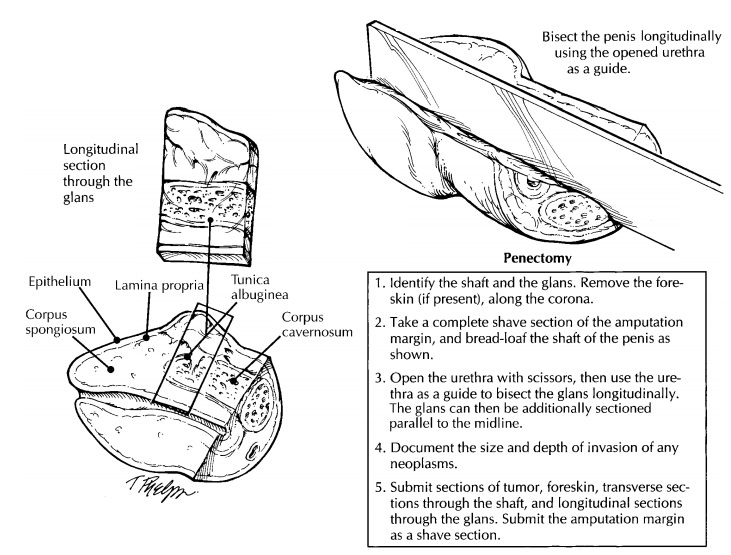
Begin
the dissection by taking a shave section from the penile shaft at the
amputation site. This section represents the only margin. If it is care-fully
taken, this section will include margins of the skin, erectile bodies, and
penile urethra. If all of these components cannot be included in a single
section, submit each component individu-ally. Remove the foreskin from the
uncircumcised penectomy. This can be done with a circular cut leaving a 5-mm
rim of foreskin attached to the corona. The foreskin should then be separately
processed according to the guidelines given pre-viously in the section on the
foreskin. The deep structures of the penis are most easily visualized when the
penis is sectioned in two different planes. Bread-loaf the shaft perpendicular
to its long axis. Begin at the proximal end of the speci-men, and stop 1 to 2
cm from the corona. Next, serially section the distal penis parallel to its
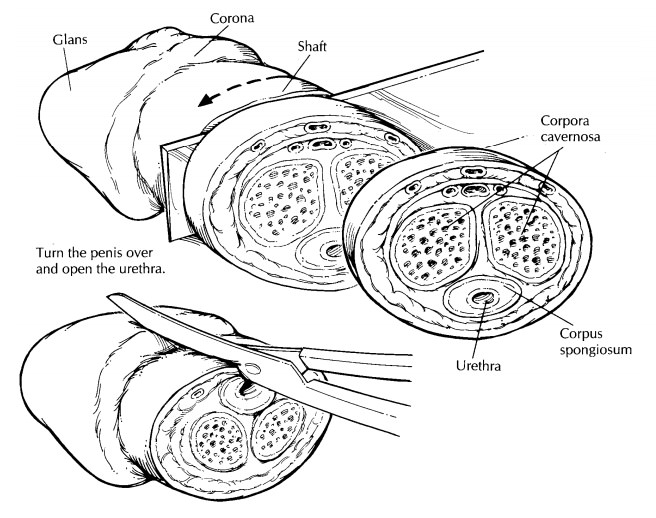
long axis. The first of these parallel longitudinal sec-tions should bisect the
proximal penis into equal halves midline through the urethra. This is not a
difficult section if you first use scissors to open the urethra at the
6-o’clock position (i.e., midventral plane), and then insert a knife into the
opened urethra to complete the longitudinal section. Serially section the rest
of the glans parallel to this initial midline cut in the sagittal plane.
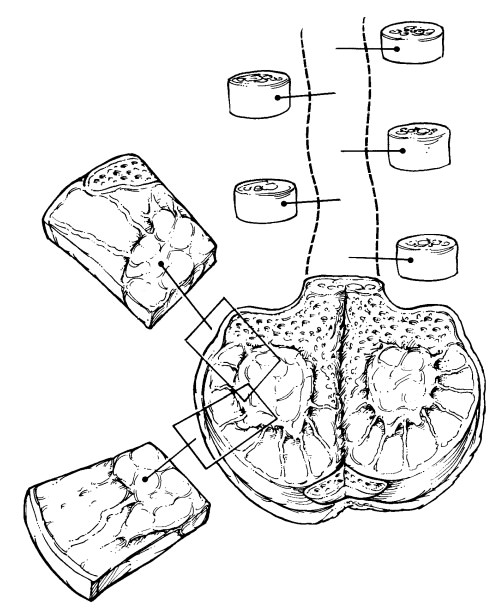
Examine
the cut surfaces of the specimen. Locate and describe the appearance of the
penile urethra and the four anatomic levels of the glans. As described by
Cubilla et al.,15 they include:
(1) the epithelium, the flat less than 1 mm layer
of epithelium covering the surface of the glans; (2) the lamina propria, the
approximately 2 mmthick layer of loose connective tissue beneath the
epithelium; (3) the corpus spongiosum (grossly reddish, spongy tissue located
between the lamina propria and the tunica albuginea) sur-rounding the distal
urethra; and (4) the corpora cavernosa (spongy reddish brown tissue encased in
a band of firm white tissue, the tunica albugi-nea). If a tumor is present,
measure how deeply it infiltrates the penis, and try to determine which of the
four anatomic structures the tumor in-volves. The standard sections that should
be submitted for histologic evaluation include the following: (1) a shave
section from the shaft margin (including the skin, erectile bodies, and
urethra); (2) sections of foreskin; (3) transverse sections through the shaft
at two or three different levels; and (4) longitudinal sections through the
glans including a midline section with the urethra. When sampling the tumor,
submit sec-tions that demonstrate its relationships to the ad-jacent surface
epithelium, to the urethra, and to the corpora spongiosum and cavernosum. For
tumors that involve the urethra, determine the maximum tumor extension by
submitting sec-tions at regular intervals along the entire length of the penis.
Important Issues to Address in Your Surgical Pathology Report on Penectomies
· What
procedure was performed, and what structures/organs are present?
· Is a
neoplasm present?
· Where is
the tumor located (e.g., foreskin, glans, shaft, and/or urethra)?
· Is the
tumor in situ or infiltrating?
· What are
the histologic type and grade of the tumor?
· What is
the size of the tumor, and how deeply (in millimeters) does the tumor
infiltrate the penis?
· Is
vascular invasion identified?
· What
deep structures does the tumor involve (e.g., lamina propria, corpus spongiosum,
corpora cavernosa, urethra, prostate, adjacent structures)?
· Are the
resection margins free of tumor?
· Does the
non-neoplastic portion of the penis show any pathology?
Related Topics