Chapter: Paediatrics: Paediatric Surgery
Paediatrics: Miscellaneous conditions
Miscellaneous conditions
Tongue-tie
Common and rarely causes symptoms.
Tongue-tie does not cause lisp, and is most definitely not responsible for
eating problems in an older child. Division of a tongue-tie does not alter the
natural history of either con-dition. Tongue-tie does affect the ability of
newborns to breastfeed and division of the lingual frenulum within the first
week of life will correct this problem. Bottle feeding is not affected.
Dermoid cysts
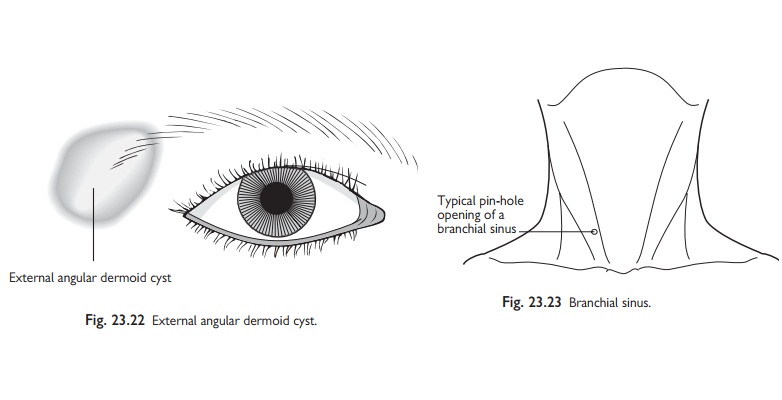
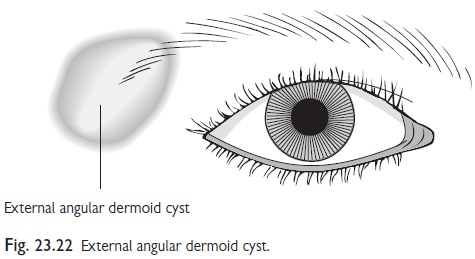
Common in children (Fig. 23.22).
Dermoids are non-tender, mobile subcu-taneous cysts filled with keratin, hair
follicles, and sebaceous glands. They enlarge slowly and should be treated by
excision. Dermoid cysts occur most frequently along lines of embryological
fusion, such as lateral corner of the eyebrows (external angular dermoid),
midline of the neck, over the bridge of the nose, and suprasternal notch.
Thyroglossal duct cysts (TDC)
Present with midline swelling in
the neck, just below the hyoid bone. The swelling rises with tongue protrusion
and swallowing. TDCs develop from epithelial remnants left after descent of the
developing thyroid from the foramen caecum at the base of the tongue. TDCs
gradually enlarge and eventually become infected, which makes excision more
difficult. Treatment is surgical removal of the central portion of the hyoid
bone along with the cyst and track.
Branchial remnants
Branchial remnants persist from
the branchial clefts during embryogenesis of the head and neck. Anomalies of
the second branchial cleft are by far the most common. They can be a cyst, a
sinus tract, or rarely a fistula.
•
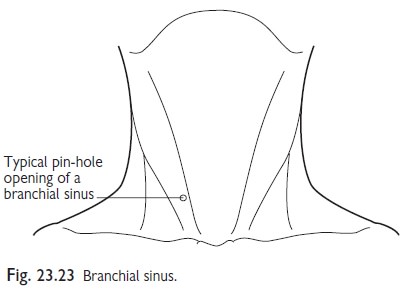
Branchial sinuses: present as small cutaneous
openings along the anterior lower
third border of the sternocleidomastoid muscle that discharge mucus (Fig.
23.23). They can communicate with the tonsillar fossa (branchial fistula).
Management is excision to prevent infection.
•
Branchial cysts: uncommon neck swellings along the
anterior border of the sternomastoid.
The differential includes cystic hygroma, which is more common, and the
treatment is surgery.
Cystic hygroma (CH)
A congenital malformation of the
lymphatic system. CHs present in early childhood as soft multilocular cystic
swellings that often appear after an intercurrent viral infection. CHs are more
often found in the neck and axillae, although they can occur anywhere,
including inside the abdomen or thorax. Large cervical cystic hygromas may
present at birth with air-way obstruction. Small CHs require no treatment.
Large lesions infiltrate the surrounding tissues making complete surgical
excision impossible. Intralesional injection of OK432 (lyophilized product of Streptococcus pyo-genes) is an
alternative to surgery in some cases.
Congenital torticollis
Within the first weeks of birth a small swelling in the baby’s neck is noticed. A sternomastoid tumour is a palpable area of fibro-sis in the lower sternomastoid muscle (SM) and is a transient phenome-non that will resolve after a few months. Sometimes there is a history of dystocia. Shortening of the SM results in torticollis with rotation and tilting of the head to the opposite side. Management is conservative in most cases with passive exercises to achieve full neck movements. Hemifacial atrophy and strabismus may develop unless full movement is restored. Occasionally it is necessary to divide the SM, but this is no substitute for physiotherapy.
Related Topics