Chapter: Paediatrics: Paediatric Surgery
Paediatrics: Gastroschisis
Gastroschisis
The incidence of gastroschisis is
1/3000 live births, but it is increasing. Most foetuses with gastroschisis are
identified on prenatal US and delivery can then be arranged in a regional
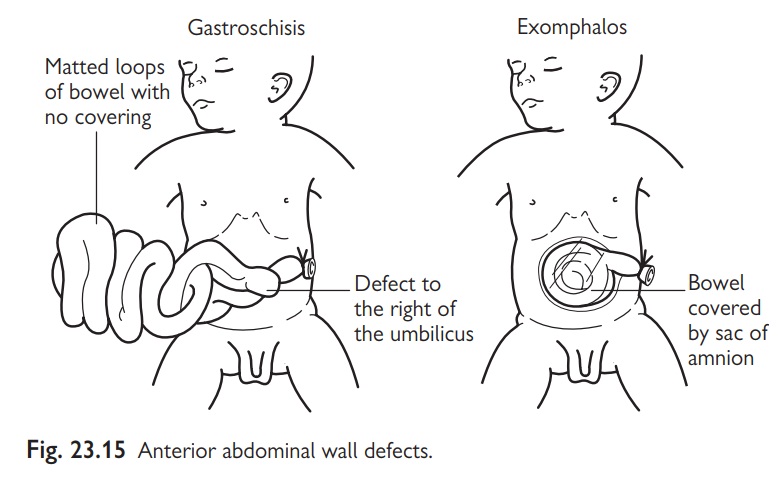
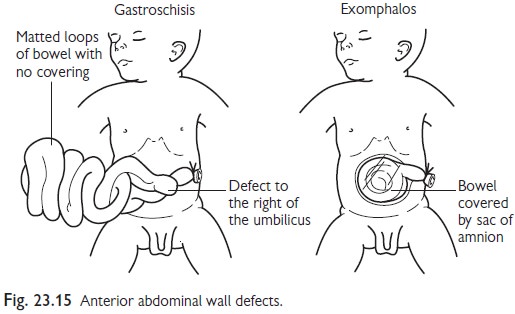
neonatal surgical centre. The abnormality is immediately apparent at birth as a
defect in the abdominal wall to the right of the umbilicus (Fig. 23.15). The
bowel is eviscerated and not covered by a sac. As a result of contact with
amniotic fluid the bowel is thickened and matted. Associated malformations are
uncommon except intestinal atresias (10%).
Management
•
Immediate:
cover the exposed bowel with Clingfilm™.
•
Keep
the baby warm and hydrated.
•
AXR is
unnecessary.
•
Surgery: the defect requires surgical
closure as rapidly as possible. Often
this has to be staged using a silo because the abdomen is too small to accommodate
the intestine. The silo is reduced serially over a period of 1–2wks and then s closure of the defect is
performed.
•
Nutrition: total parenteral nutrition may be
required for many weeks because
intestinal function is slow to resume after the abdominal wall is closed.
However, the long-term outcome is excellent.
Related Topics