Definition, Classification, Functions, Food Sources, Deficiency | Nutrition - Micronutrients | 11th Home Science : Chapter 5 : Nutrition
Chapter: 11th Home Science : Chapter 5 : Nutrition
Micronutrients
MICRONUTRIENTS
Until the middle of the 19th
century the importance of minerals and vitamins was not given adequate
emphasis. It was observed that the macronutrients alone were not sufficient to
promote and sustain growth.
This led to the discovery of the
micronutrients namely the minerals and vitamins which are essential for growth
and maintenance. Macro minerals are those which are present at levels more than
0.05 percent in the human body. Calcium, Phosphorus, magnesium, sodium and
potassium belong to this category. Other minerals present at less than 0.05
percent in the human body are defined as micro min-erals. The micro minerals
are also known as the trace elements. Some micro miner-als are iron, iodine,
zinc, copper, fluorine, selenium, chromium, manganese, cobalt and molybdenum.
1. Minerals
The minerals calcium, phosphorus, iron iodine,
sodium and others are found in various foods in combination with organic and
inorganic compounds. Minerals are necessary for body building, for building
bones, teeth and structural parts of soft tissues.
(i) Calcium
Distribution: Calcium makes up between 1.5 to 2 percent of body weight accounting for 1200-1600
g of the adult male body. Ninety percent of calcium is found in min-eralized
tissues such as bones and teeth as calcium phosphate and calcium carbonate. The
remaining 1% is found in blood, extracellular fluid (ECF), muscle and tissues.
Functions: The functions of
cal-cium in humans are manifold:
•
Bone formation: The import-
ant minerals within bone are calcium phosphate
and magne-sium. There is 1 kg of calcium in the adult skeleton as a complete
crystalline material with phos-phate.
·
Tooth formation: The enamel and dentin of tooth contain considerable amounts of cal-cium
which are dense and are present along with keratin.
Growth: It
is required for growth as it forms an important part of
the bones and teeth and proper functioning of every cell in the body.
·
Blood clotting: Calcium con-tributes
to clotting of blood.
·
Contraction of the
muscle:
Calcium ions are bound by the electrostatic
forces to the pro-teins inside and outside the cells and to cell membranes.
Proteins bound by calcium alter their configuration at the neuro muscular
junction by the nerve impulses causing free calcium to be released. The free
cal-cium bound to troponin leads to an internal trigger and so the contraction
of the muscle takes place
·
Metabolic essentiality: Cal-cium acts as a
activator for the enzyme renin present in gastric juice which aids the
digestion of milk.
Food sources: Calcium is present in both animal and plant foods. The richest source of calcium
among animal foods is milk and among
Among the green leafy vegetables, amaranth, fenu-greek and
drumstick leaves are rich sources of calcium. Ragi among cereals is a rich
source of calcium. Small dried fish, nuts and oil seeds like gingelly seeds,
betel leaf with slaked lime are also a rich source.
Absorption:
• Factors increasing absorption of calcium: Vitamin D, acidity of digestive mass, lactose, protein and phosphorus are the factors
which favor the absorption of calcium.
• Factors decreasing absorption of calcium: Oxalic acid, phytic
acid, high fat diets including steatorrhea, emotional instability,
increased gastrointestinal mobility, lack of exercise, ageing, caffeine and
drugs decrease the absorption of calcium in the body.
Health Problems/ Deficiency:
·
Osteoporosis: This is a condi-tion
associated with a loss in bone density and bone mass which literally means
“porous bone”. With the ageing process resorption predominates bone formation
resulting in osteopo-rosis.
Risk factors for osteoporosis include
·
Females who are fair complexioned are at eight times more at
risk
·
Asian Race
·
Family history
·
Prolonged dietary insuf-ficiency
·
Poor absorption and uti-lization of calcium
·
Restricted movement
·
Decreased levels of estro-gen
·
Hyper parathyroidism
·
Vitamin D sufficiency
·
Osteomalacia: It is a condition where the quality of the bone is diminished and the quantity of
the bone is not compromised.
·
Osteopenia: It refers to the bone density that is lower than nor-mal peak density but not low
enough to be classified as osteoporosis. The difference between osteopenia and
osteoporosis is a matter of severity of the loss of bone density.
·
Tetany: A decrease in serum calcium levels gives rise to a condition called tetany. The
symptoms of tetany are severe intermittent spasms of the mus-cles of hands and
feet accompa-nied by muscular pain. Twitch-ing of facial muscles occurs.
(ii) Phosphorus
Distribution: It comprises 1
per-cent of total body weight along with calcium. An adult human body contains
about 400-700 g of phos-phorus as phosphates. Bones and teeth contain 85
percent of phos-phorus and soft tissues contain15 percent of phosphorus.
Functions:
·
Formation of bone and teeth along with calcium and magnesium.
·
Formation of phospholipids which are integral parts of cell
structure.
·
Constituent of co enzymes like coenzyme I and co – carboxylase.
·
Integral constituent of DNA and RNA (nucleic acids) and
nucle-oproteins.
·
Buffering of acid or alkali excesses to maintain normal pH.
·
Temporary storage and transfer of the energy derived from
met-abolic fuels.
·
As part of enzymes needed for the metabolism of carbohy-drates,
protein and fats.
Food Sources: Phosphorus is widely distributed in
foods. Milk and meat are rich in phospho-rus. Whole grain cereals, legumes,
nuts, carrots and fish are also rich sources of phosphorus.
Calcium Phosphorus ratio: Nutri-tionists
recommend that a Ca:P ratio between 1:1 to 2:1 should be provided by
the total diet.
Deficiency: Phosphorus is so ubiquitous in various foods that near total starvation is
required to produce dietary phosphorus deficiency. Inadequate phospho-rus
intake is expressed as hypo-phosphatemia which manifests in the form of anemia,
anorexia, muscle weakness, bone pain, rickets, osteomalacia, general weakness
and increased susceptibility to infection.
(iii) Iron
Distribution: Iron content of nor-mal adult man is estimated
to be about 4 grams. Iron is distributed as 60% in the circulating hemoglobin, 5% myoglobin, various heme and non heme enzymes (5%). The remaining iron is
found in body storage as ferritin (20%) and hemosiderin (10%) the two major iron storage proteins
Forms of dietary iron
·
Heme iron: Heme iron is the iron associated to the protein globin to form hemoglobin and is found
in flesh foods only
·
Non heme iron: This form is pres-ent
in all plant sources in addition to 60% of animal sources.
·
Absorption: Several factors favor and inhibit iron absorption
Factors favoring absorption of Iron:
·
Body needs,
·
Ascorbic acid,
·
Animal tissues,
·
Pregnancy,
·
Low iron status,
·
Low heam iron intake.
Factors decreasing the absorption of iron:
·
Binding agents like fiber, phos-phates, phytates and oxalates,
·
High calcium intake,
·
Achlorohydria (low gastric acid)
·
Infection
·
Gastrointestinal disease.
Functions: Iron has varied
signif-icant functions in human body. They include:
·
Transport and storage of oxygen where each gram of hemoglobin
contains about 3.34 mg of iron.
·
As myoglobin iron is required for oxygen storage in muscle.
·
Iron acts as a cofactor of enzymes.
·
It is a component of cell enzyme systems that oxidize glucose
and other energy yielding nutrients.
·
Production of immune cells that attack foreign bacteria invading
the body.
·
Positive iron balance is neces-sary for continued growth.
·
To build reserves for physio-logic stress during adolescence for
both boys and girls.
·
Necessary for brain develop-ment, cognitive function, the
synthesis and breakdown of neurotransmitters.
Food sources:
Rich sources of iron
are cereals, millets, pulses and green leafy veg-etables. Of the cereal grains
and millets bajra and ragi are very good sources of iron. Other sources of
plant foods include manathakali leaves, rice flakes, mint, soya bean, cow pea,
gingelly seeds and dates. Animal food sources include red meat, and fishes like
herring and mackerel
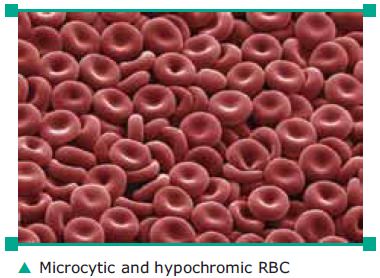
Deficiency
·
Iron Deficiency anemia: When there is an insufficiency of iron for the formation of
hemoglobin, the RBC’s become pale and small. The resulting anemia is called
hypo-chromic and microcytic anaemia which is the most common form of anaemia
throughout the world affecting women mainly in their reproductive years,
infants and children.
Causes: Low iron intake, blood loss, malabsorption
chronic dis-eases, obesity
·
Regular consumption of iron rich foods, vitamin C rich foods,
seasonal fruits and vegetables can definitely prevent anemia.
(iv) Iodine
Distribution: It is one of the
essen-tial micronutrients required for normal growth and development of human
brain and body. Human body contains a total of 15-20 mg of iodine. Thyroid
gland contains 75% of iodine and is an essential constituent of thyroxine the
active principle of thyroid gland
Functions: Iodine though required in small quantities is needed to per-form the following
functions
·
Synthesis of thyroxine which regulates growth, development and
reproduction.
·
Helps the thyroid hormones to increase and regulate the
pro-cesses of brain function
·
Enables the thyroid hormones to regulate the conversion of
carotene to active vitamin A.
Food sources:
Marine fish and eggs are good sources of
iodine. Based on the dietary pat-tern and analysis of raw foods, iodine content
of various regional diets range from 170-300 μg/ day
Deficiency: It covers a collection of disorders at all stages of human growth and development.
·
Goiter: Goiter is the
enlargement of thyroid gland which
results when iodine is not available in sufficient quantities to produce normal
quantity of thyroxine. It also arises from eating foods (goitrogens) that
inhibit the synthesis of thyroxine

·
Cretinism: A congenital disease resulting from a lack of iodine and thyroxin secretion
characterized by physical deformity, dwarfism, men-tal retardation and often
goiters.
·
Dietary improvement: Salt iodiza-tion
remains the most cost effec-tive way to deliver iodine to both humans and
livestock and is cred-ited with eradicating iodine defi-ciency.

(v) Zinc
Distribution: Zinc is the most important intracellular trace element. An adult human contains
2g of zinc of which 60% is in skele-tal muscle, 30% in bone and 4-6% is present
in zinc.
Functions: The functions of zinc include
·
Important constituent of enzymes like alkaline phospha-tase and
carbonic anhydrase.
·
Required by protein kinases that participate in gene expression.
·
Also a component of metallo-enzymes.
Food sources: Meat, seafood and liver are good sources
of bioavail-able Zinc. In cereals most of the zinc is found in the outer fiber
rich part of the kernel.
Deficiency: The clinical manifes-tations of severe zinc deficiency in humans
are growth retarda-tion, dermatitis, hair loss, diarro-hea, increased
infections, delayed wound healing, loss of appetite, hypoguesia (diminished
taste) dys-guesia (altered taste) hyposmia (diminished smell). Decreased zinc
intake is associated with increased risk of low birth weight and preterm
delivery.
2. Vitamins
Fat soluble vitamins A, D, E and K and also water-soluble
vitamins C and B group are found in foods. These are needed for growth, normal
function of the body and normal body processes.
2. a. Fat Soluble Vitamins
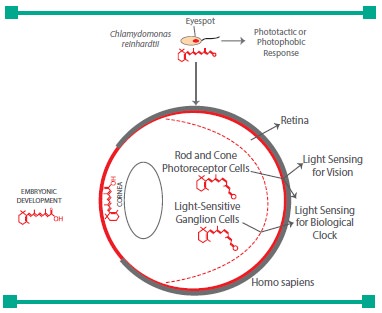
(a) Vitamin A:
The vitamin A compounds include retinol, retinal and retinoic acid. Because it has a
specific function in the retina of the eye and because it is an alcohol it was
given the name ret-inol. Beta carotene is precursor of vita-min A and is found
in large quantities in vegetables and fruits.
Functions: Vitamin A performs the following
functions:
·
Vitamin A is essential for vision in normal and dim light.
·
Formation and maintenance of healthy functioning epithelial
tissue.
·
Glycoprotein and mucoprotein synthesis
·
Cancer prevention
·
Prevention of degeneration of myelin sheath
·
Normal bone formation and reproduction.
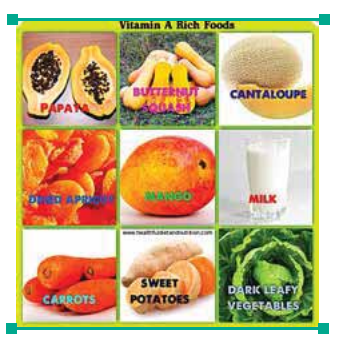
Food sources: In the animal foods vitamin A is present
in the form of retinol which are identified to be liver, cream, butter and egg
yolk. Liver oils of fish like cod, halibut and shark are the richest sources of
vitamin A. The main contribu-tors of beta carotene are the yellow and green
vegetable fruit sources of carotene- carrots, papaya, mango, sweet potatoes,
spinach and broccoli.
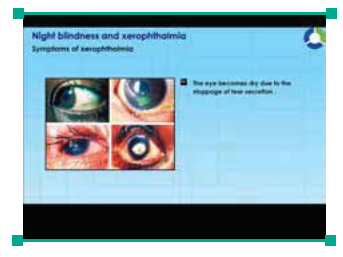
Deficiency: Decreased Vitamin A intake leads to vision problems
·
Night blindness: People suffering from
night blindness cannot see
objects in dim light
·
Xerosis Conjunctiva: The conjunctiva is dry, thickened, wrinkled
and pigmented. This is due to the keratinization of the epithelial cells.
·
Xerosis Cornea:
This man ifests in the form of corneal dryness
which gives the cornea a dull hazy and lusterless appearance.
·
Bitot’s spots: These are grey-ish or
glistening white plaques occurring in the conjunctiva usually triangular in
shape and are found in children.
·
Keratomalacia: When Xerosis of the conjunctiva and cornea is not treated it may develop into
the condition called ker-ato malacia which is character-ized by necrosis,
ulceration and bacterial invasion of cornea leading to the total destruction of
the eyeball and eventually total blindness.
Prevention of vitamin A deficiency
The strategy should be
a combina-tion of long term nutrition educa-tion programme, enhanced intake of
vitamin A rich food, improve-ment in household food security and availability
of vitamin A rich foods and a periodic massive dose of vitamin A.
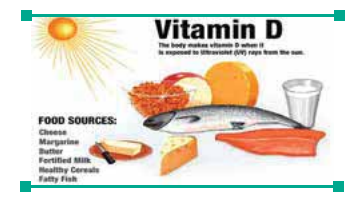
(b) Vitamin D:
Vitamin D is known to
be a prohormone of a sterol type and the synthesis of active form
of vitamin D is known as the 1,25 – dihydroxycho-lecalciferol which is
accomplished by the combined action of skin, liver and kidneys.
Functions
·
Maintains balance with para-thyroid hormone to stimulate the
active transport of calcium and phosphorus.
·
Acts on the bones promoting calcification.
·
Facilitates the absorption of calcium and phosphorus from the
intestines.
Involved in widespread basic cell processes
with targets in brain, kidney, liver, skin, repro-ductive tissues.
Food sources: Vitamin D is pres-ent only in some foods of
animal origin. Certain marine fishes and fresh water fishes are known to be
good sources of vitamin D. The most important sources are egg yolk, butter, cheese,
milk.
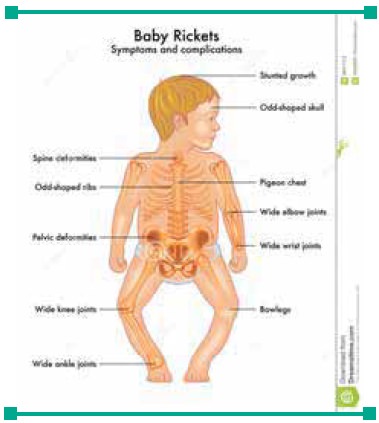
Deficiency: Vitamin D deficiency occurs in children who
are not ade-quately exposed to sunlight. It is characterized by inadequate
min-eralization of the bone. In children the condition is known as rickets and
in adults it is called Osteoma-lacia.
Rickets: In rickets there is
soft-ening of the skull bones and the head is enlarged, elongated and flattened
on the vertex. Softening of the ribs, sinking of the chest, beaded junctions of
the ribs with cartilages (rickety rosary), pigeon chest, knock knees and bow
legs. Deformities of the long bones spine, pelvis, muscles, and feet are
observed. Dentition is delayed.
Osteomalacia: It is the adult counterpart of
rickets. It occurs in
Besides it is
found among those who stay indoors all day and seldom go out in the sun.
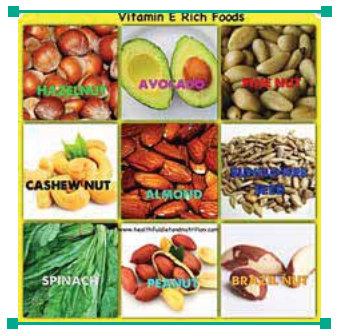
(c) Vitamin E:
Vitamin E is the generic name for a group of vitamins, three of which –alpha tocopherol,
beta tocopherol and gamma tocopherol display the greatest biologic activity. Of
these three, alpha tocopherol is the most significant form of Vitamin E
·
Functions
·
Vitamin E a major antioxidant which reduces the incidence of
heart diseases.
·
It is essential for normal repro-duction in man.
·
It acts along with selenium in reducing the body’s require-ment
for each other.
·
It plays a vital role in the immune function of the body.
Food sources: Vegetable oils, nuts and whole grams are the richest sources of vitamin E (eg. Wheat
germ oil). It is present in small quan-tities in lettuce, grasses and embryos
of many seeds. In general, plant foods are richer sources of vitamin E than
animal foods.
Deficiency: Vitamin E deficiency has been associated with irritabil-ity, edema and hemolytic
anemia among infants. Also Muscular dys-trophy is common to all species in
which there is degeneration of skel-etal and cardiac muscle with vita-min E
deficiency.
(d) Vitamin K
Vitamin K occurs in two forms.
·
Phylloquinones (vitamin K1) - plant source and dietary form of
vitamin K
Menaquinone (vitamin
K2) - syn-thesized by intestinal bacterial flora.
Functions: The major functions of Vitamin K though not many are listed as follows:
·
Vitamin K is essential for blood clotting.
·
Required for the synthesis of blood clotting factors by the
liver.
·
Vitamin K is vital to maintain normal levels and activation of
blood clotting factor like prothrombin,
Food Sources:
The major dietary
source of vita-min K is Phyllo Quinone which is present in high concentration
in most vegetables like cabbage, spin-ach and cauliflower. Animal food sources
include cheese, egg yolk, and liver.

Deficiency: It manifests in the form of defective blood
clotting. Low levels of prothrombin and hemor-rhage are seen in severe forms of
deficiency.
2.b. Water Soluble Vitamins
(a) Thiamin (B1):
Thiamin is the first member of the B complex vitamins which is essential to the body
in its coenzyme form.
Functions: The coenzyme of thi-amin is Thiamin Pyro Phosphate (TPP).
Thiamin is useful in our body for the following functions
·
It enhances growth in human beings.
·
It plays an important role as a coenzyme in carbohydrate
metabolism
·
Maintenance of nerves in nor-mal condition.
Food sources: Good food sources include lean pork,
beef, liver, whole or enriched grams and legumes.
Deficiency of thiamin: The dis-covery of thiamin provided the answer
to the puzzle of a nutri-tional problem called beri beri. The deficiency of
thiamin causes beri beri in human beings. The Philip-pino word beri beri means
“I Can’t” refers to the lack of neuromotor coordination in persons with the
disease.
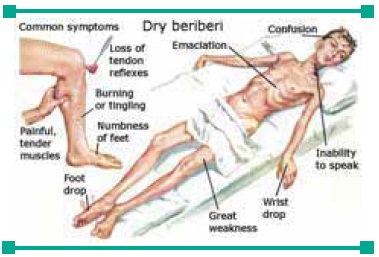
Beri Beri is of two types: dry and wet type. In dry beri beri the mus-cles become progressively wasted, weak and walking becomes dif-ficult. If not treated the patient becomes bedridden and will die. In wet beri beri edema is present which involves the face, trunk and serous cavities. Palpitation and breathless-ness are present. The heart becomes weak and death occurs due to heart failure. Infantile beri beri is seen in many South East Asian countries where the diets consist mostly of “polished rice”.
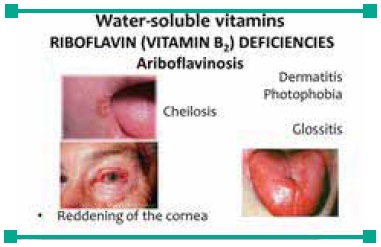
(b) Riboflavin (B2):
Riboflavin is a sta-ble vitamin which is
resistant to acid, heat and oxidation. But it is unstable in the presence of
alkali and light.
Functions:
The two coenzymes of Riboflavin Flavin Mono
Nucleotide (FMN) and Flavin Adenine Dinucleo-tide (FAD) perform the following
functions
·
Formation of red blood cells in the bone marrow.
·
Regulates the functions of hor-mones in carbohydrate
metab-olism.
·
Present in the retina in the free form which gets converted to a
compound which stimulates the optic nerve.
·
Release of energy from glucose, amino acids and fatty acids.
Food sources: Good sources of riboflavin are milk
and milk prod-ucts, eggs, liver, whole or enriched grains and green leafy
vegetables.

Deficiency: The deficiency of riboflavin
(ariboflavinosis) leads to glossitis (swollen and reddened tongue), swollen
lips, cheilosis (inflammation of the corners of the mouth, are some of the com-mon
symptoms observed. Further deficiency states are marked by chronic conditions
like tubercu-losis, prolonged fevers, malab-sorption, Hyperthyroidism and
malignancy.
(c) Niacin:
Niacin formerly known as nic-otinic acid was
obtained by the oxida-tion of nicotinic acid. Apart from the food sources,
Niacin is also obtained from tryptophan (60mg) an essential amino acid which
can be converted into niacin (1mg).
Functions: Two coenzymes of Nia-cin Nicotinamide Adenine Dinu-cleotide
(NAD) Nicotinamide Adenine Dinucleotide Phosphate (NADP) are required for:
·
Release of energy from all energy yielding nutrients like
carbohydrate, protein and fat.
·
Normal functioning of the skin, intestinal tract and the nervous
system.
·
Synthesis of protein and fat for the formation of DNA and RNA.
Food sources: Whole cereals, pulses, nuts and meat
are good sources of Niacin. Groundnut is rich in Niacin. Milk is rich in
Tryp-tophan the precursor of Niacin in the body.
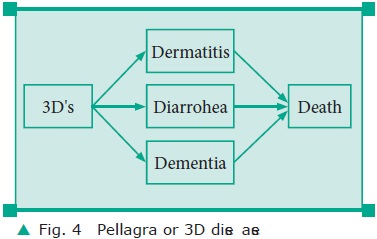
Deficiency: Deficiency of Niacin causes Pellagra which
is the 3D (Dermatitis, diarrohea, dementia or depression) disease leading to
the fourth D (Death).
Consumption of diets
rich in corn can create amino acid imbalance as corn is rich in leucine and
deficient in tryptophan. The typical features of pellagra are loss of weight
and increasing weakness. Non- specific signs like anorexia, nausea, diges-tive
disturbances and emotional changes like anxiety, irritability and insomnia may
be present.

(d) Pyridoxine (B6):
Pyridoxine exists in the body in three forms:
Pyridoxal, Pyridoxine and Pyridoxamine. Pyri-doxal 5 phosphate is the co-enzyme
form of pyridoxine.
Functions: Pyridoxal 5 phosphate acts as a coenzyme in protein metabolism. Its functions include
·
Amino acid transport.
·
Essential for the growth of infants.
Food sources: Good food sources include grains, seeds,
liver, kidney and other meats.

Deficiency: Clinical Symptoms of pyridoxine deficiency have not been clearly defined. Some
types of angular stomatitis (cracking at the corners of the lips) and cer-tain
types of anaemia have been reported due to decreased intake of pyridoxine.
(e) Folic acid:
The term folic acid was coined to as it was first extracted from dark green leafy
vegetables such as spinach.
Functions: The different
func-tions of folate include:
·
Normal growth and division of all cells.
·
Maturation of red blood cells.
·
Vital role in the metabolism of some amino acids.
Food sources: The rich sources of folate are fish,
mutton, liver, egg, chicken, green leafy vegetables and pulses.
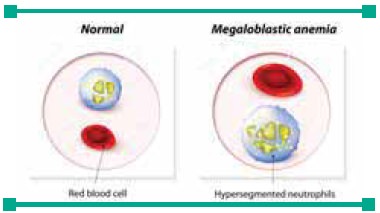
Deficiency: Deficiency of folic acid causes megaloblastic anae-mia. Megaloblasts appear in bone marrow and peripheral blood. Poor dietary intake of folic acid, low absorption, increased losses, increased requirements, infes-tation, infection and drugs also cause folic acid deficiency. Symp-toms include weakness, tiredness, dyspnea, sore tongue, headache and palpitation. Folate deficiency during pregnancy can result in neural tube defects like spina bifida and anencephaly.
(f) Cyanocobalamin (B12):
The vitamin is named as
cyanocobalamin because of the presence of cobalt and cyanide in its structure.
It can be absorbed in the body only in the presence of Intrinsic Factor (IF).
Functions: Physiological func-tions and biochemical functions of
cyanocobalmin are:
·
Maturation of erythrocytes
·
Synthesis of myelin (white sheath of lipoprotein) that
sur-rounds many nerve fibres.
·
Increase in White Blood Corpus-cle (WBC) count and platelet.
·
Stimulation of appetite and general wellbeing of the people.
·
Cures neurological symptoms of pernicious anemia.
Food sources: Cyanocobalmin is synthesized by
bacteria and is found in foods of animal origin. Liver is the richest source of
cya-nocobalmin. Meat, fish, kidney, brain and eggs are good sources of
cyanocobalmin.

Deficiency: Inability to produce the intrinsic factor
which binds cyanocobalmin leads to perni-cious anemia. The red blood cells are
macrocytic and the count is often less than 2.5 million. Symp-toms include
soreness and inflam-mation of the tongue, paresthesia (numbness and tingling)
in fingers and toes, demyelination of the white fibres of the spinal cord and
in severe cases degeneration of the spinal cord.
Other B complex vitamins include biotin,
pantothenic acid which do have their vital functions as coen-zymes in various
biochemical func-tions of the body
(g) Vitamin C (Ascorbic acid):
Ascorbic acid is the chemical
name of vitamin C which can be synthesized from glu-cose but humans depend on
their diet for vitamin C as they do not have an enzyme gulonolactone oxidase
which catalyzes the conversion reaction.
Functions: Functions of vitamin C include:
·
Collagen formation of bone, teeth, cartilage, skin and scar
tissue.
·
Formation of dentin layer of tooth
·
Wound healing.
·
Activation of calcitonin, gas-trin, oxytocin, thyrotropin,
vasopressin.
·
Drug detoxification
·
Regulation of cholesterol, maintenance of the blood ves-sel
structure and antioxidant effects.
·
Conversion of inactive form of folic acid into its active form
·
Reducing agent to keep iron in its ferrous form to facilitate
iron solubility.
·
Adrenal cortex function.
·
Enhances calcium absorption.
Food Sources: Citrus fruits like orange, lemon,
tomatoes, guava, watermelon are good sources of Vitamin C
Deficiency: Scurvy the most severe form of vitamin C
deficiency arises mainly due to faulty cooking habits and inadequate intake of
fruits and vegetables. The clinical features of scurvy are characterized by
gin-givitis (bleeding gums) petechiae (small hemorrhagic spots), arthral-gia
(pain in the joint), depression, postural hypotension, delayed wound healing.
Main deficiency symptoms in infants include tender bones, cessation of bone
growth, anaemia and pyrexia.

Related Topics