Chapter: Surgical Pathology Dissection : The Cardiovascular, Respiratory System
Lungs Pleural Resections for Malignant Mesotheliomas: Surgical Pathology Dissection
Pleural Resections for Malignant Mesotheliomas
The
diagnosis of malignant mesothelioma is usu-ally established on the basis of
cytologic material or small incisional biopsies. Rarely, malignant
mesotheliomas are resected in an attempt to obtain a surgical cure. For tumors
arising in the chest, these specimens generally consist of lung with en bloc
removal of any adjacent involved mesothelium-lined structures such as the
parietal pleura of the chest wall, the pericardium, and the diaphragm. These
specimens can generally be handled using the same principles guiding the
dis-section of other lung specimens, as detailed above. When it comes to
malignant mesotheliomas, how-ever, a few points warrant special emphasis.
1.
Immunohistochemistry and electron mi-croscopy
have become important adjuncts to routine microscopic evaluation in the
diagnosis and classification of malignant mesothelioma. For lung specimens with
pleura-based tumors, always consider the possibility of a malignant
mesothelioma, and process a small portion of the tumor for electron microscopy
should this mod-ality be needed to establish the diagnosis.
2.
Because of the variable and sometimes
deceptively bland histopathologic appearance of maligant mesotheliomas, the
diagnosis and classification are aided by ample sectioning for histologic
evaluation. Suspected malignant meso-theliomas should be sampled much more
exten-sively than the conventional lung carcinoma. For smaller lesions, submit
the tumor in its entirety. For large lesions, submit at least one section per
centimeter of tumor.
3.
Depending on the extent of tumor involve-ment
along mesothelium-lined surfaces, these resections may be anatomically complex.
Do not
Instead, take the time necessary to orient the
specimen, identify all structures present, document the extent of tumor spread,
and locate each margin (e.g., bronchus, pulmonary vessels, chest wall,
diaphragm) for histologic evaluation.
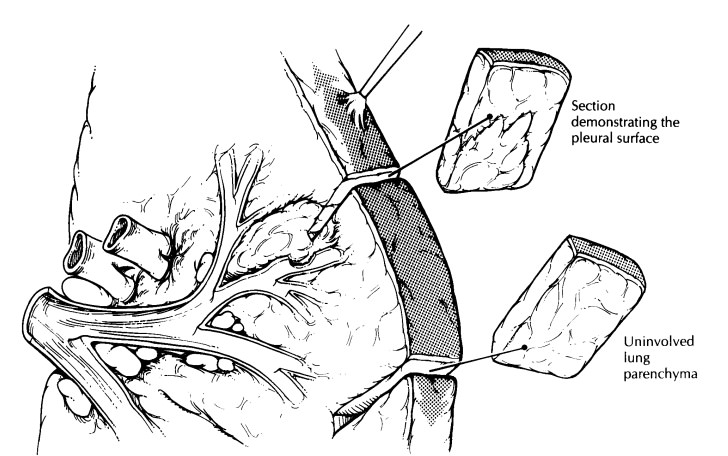
4. Submit
additional sections of uninvolved lung, and evaluate them for the presence of
ferru-ginous bodies, pleural plaques, and interstitial fibrosis.
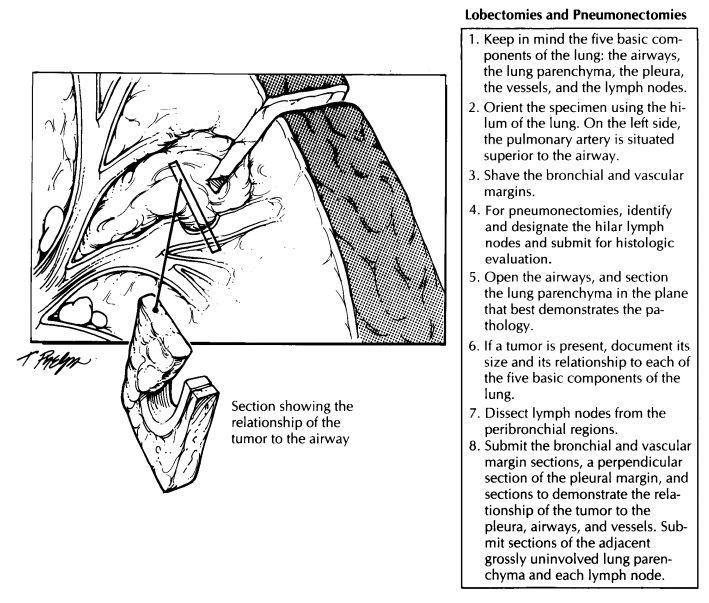
Important Issues to Address in Your Surgical Pathology Report on Lung Resections
·
What procedure was performed, and what
structures/organs are present?
· Is a
neoplasm present?
· How
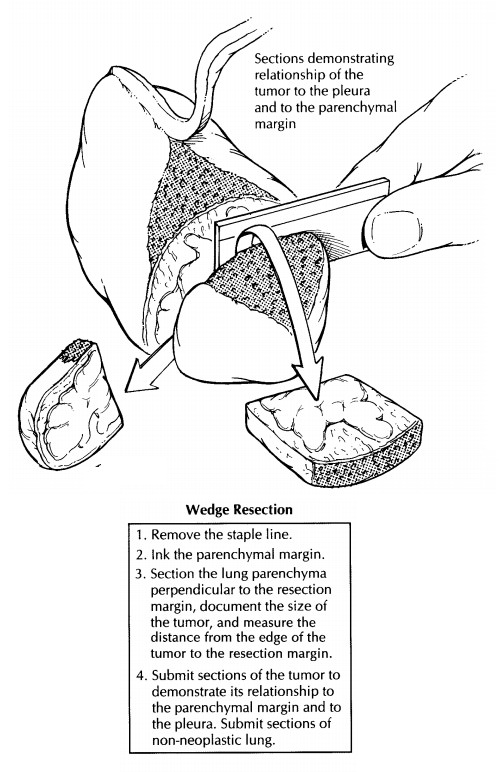
large is the tumor, and where is it located?
· What are
the histologic type and grade of the tumor?
· Does the
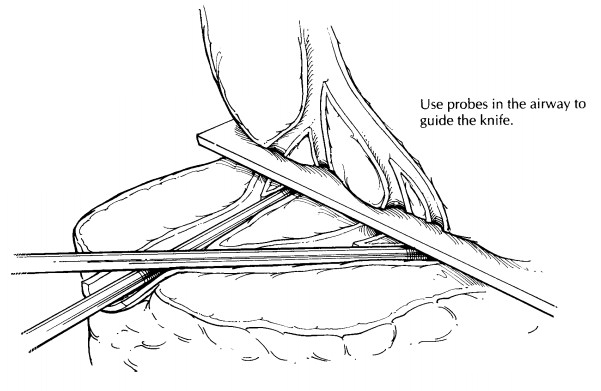
tumor infiltrate the large airways, pleura, or vessels?
· What is
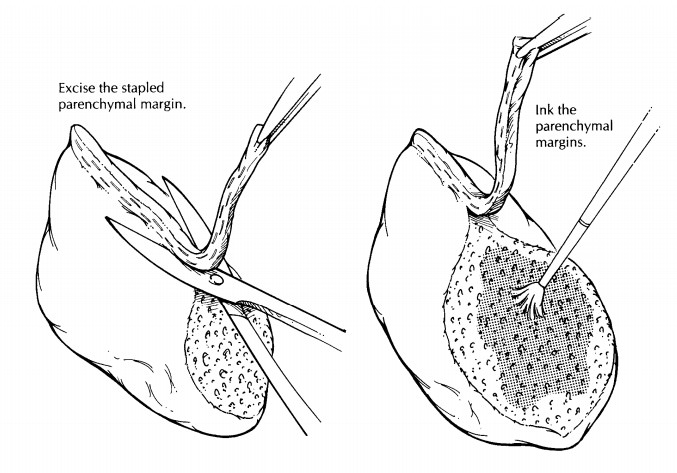
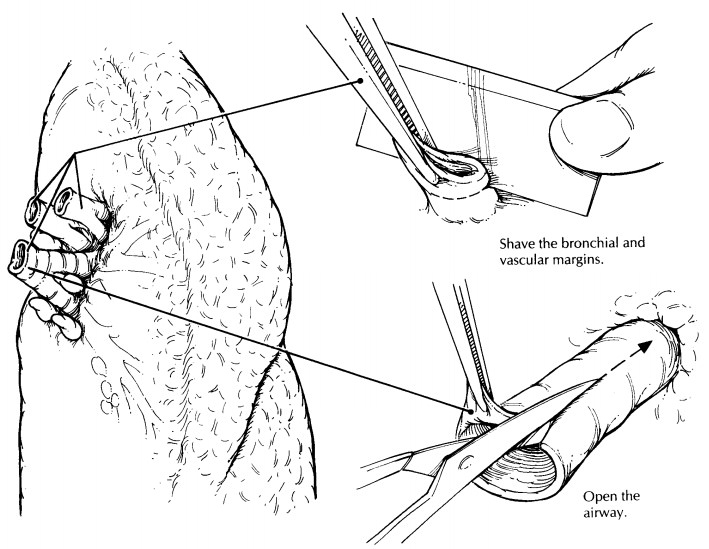
the status of each of the margins (paren-chymal, vascular, and bronchial)?
· Does the
tumor involve the lobar or main-stem bronchi?
· Is there
any evidence of metastatic disease? Record the number of lymph nodes examined
and the number of lymph node metastases. If nodal involvement is only by direct
extension, this feature should be noted.
·
Is there any pathology in the non-neoplastic
lung (e.g., granulomas, postobstructive pneu-monia)?
Related Topics