Chapter: Surgical Pathology Dissection : The Cardiovascular, Respiratory System
Lung Lobectomies and Pneumonectomies: Surgical Pathology Dissection
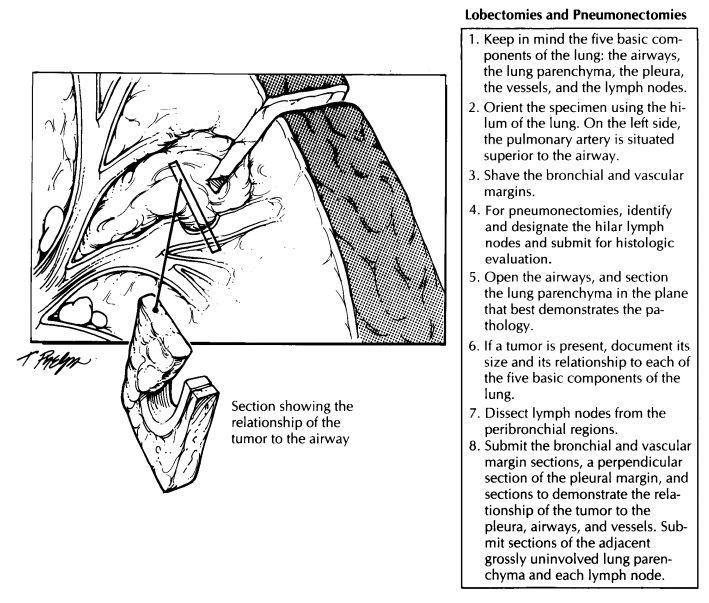
Lobectomies and Pneumonectomies
The
largest lung specimens consist of lobecto-mies and pneumonectomies. These
procedures are usually done to remove neoplasms, although pneumonectomies for
non-neoplastic lung dis-ease are encountered in some medical centers performing
lung transplantations. When a tumor directly invades beyond the pleura, these
specimens may also include an en bloc resection of the involved adjacent
structures (e.g., chest wall, left atrium, or diaphragm).
Weigh,
measure, and anatomically orient the specimen while it is fresh. One quick and
easy way to orient the specimen is to inspect the struc-tures at the lung
hilum. On the left side the pul-monary artery is situated superior to the
airway, while on the right side it is situated anterior to the airway. Also,
the right side has three lobes, whereas the left side has two and a prominent
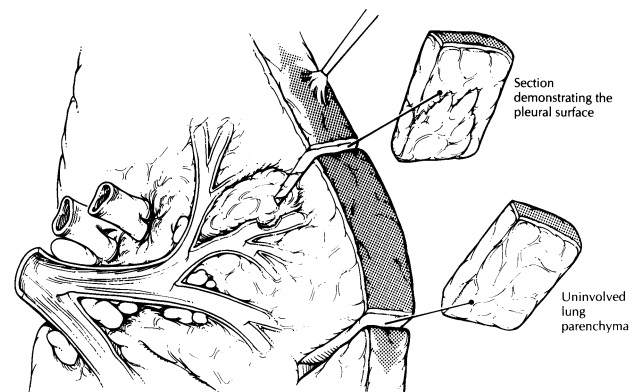
lingular segment. Carefully inspect the pleural surfaces. Look for the presence
of pleural retrac-tion, because this finding suggests the presence of an
underlying neoplasm. Palpate the intact specimen: Is the tumor located
centrally or pe-ripherally? Which lobe of the lung appears to be involved? Does
the tumor extend across a fis-sure to involve more than one lobe?
The lung
may be processed in either the fresh or the fixed state. If immediate
dissection of the specimen is not required, it is best to fix the speci-men in
distention. Infuse formalin directly into the large airways, and submerge the
entire speci-men in formalin for overnight fixation. Take care not to
overdistend the lung.
If you
remember each of the five basic compo-nents of the lung (airways, lymph nodes,
vessels, parenchyma, and pleura), then your description and dissection can be
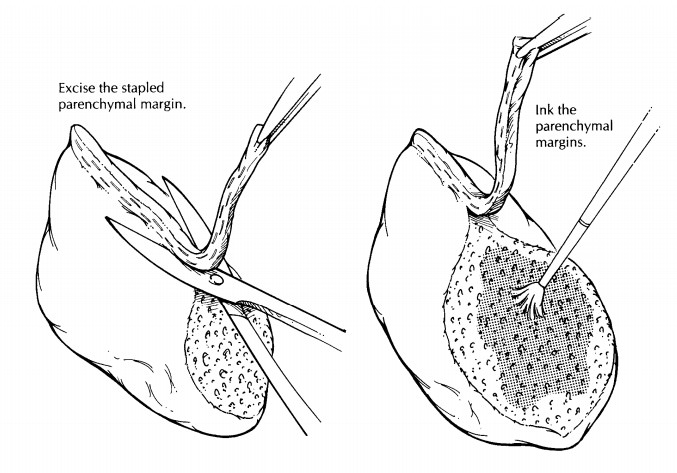
carried out in a simple and systematic fashion. Many proximal lung tumors arise
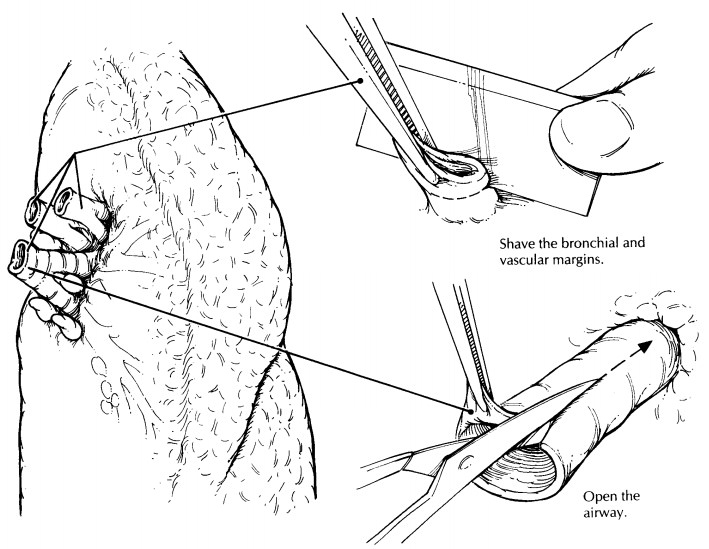
from the airways, and so we find it most helpful to start the dissection with
the airways. Begin by removing the bronchial and vascular margins as shave
sections. Next, expose the bron-chial mucosa by opening the large airways out
to the subsegmental branches with small scissors. Carefully examine the mucosa
of the airways, because subtle changes in the appearance of the mucosa may
indicate a premalignant lesion. Similarly, open the large pulmonary vessels and
evaluate them for invasion by tumor.
By
dissecting the larger airways, you have op-portunely exposed the regional lymph
nodes, and these should be sampled at this time. Direct the search for lymph
nodes to the soft tissues at the hilum and to the lung parenchyma immedi-ately
surrounding the airways. Lymph nodes are often easily visualized by their black
(anthracotic) pigmentation. It is generally not necessary to fur-ther designate
these peribronchial lymph nodes. The status of the various mediastinal lymph
node groups is crucial to the staging of lung tumors. These lymph node groups
are usually separately submitted and labeled by the surgeon, although
pneumonectomies may be accompanied by at-tached hilar lymph nodes. Such lymph
nodes should be identified by their location in the hilum of the lung and
specifically designated “hilar lymph nodes.”
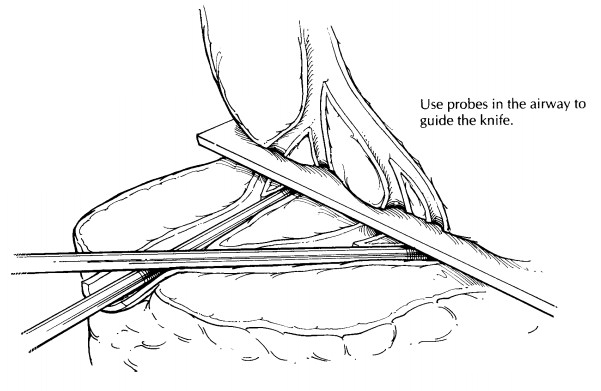
Section
the lung parenchyma in the plane that best reveals the pathologic process and
its relationship to the surrounding structures of the lung. For proximal lung
tumors, this relationship can best be demonstrated by sectioning the lung along
the plane of the involved airways. As illus-trated, this can be accomplished by
first placing probes into the airways that have already been partially opened
and then using these probes to help guide your knife through the lung
paren-chyma. In this manner, one can determine the origin and size of proximal
tumors and evalu-ate the lung parenchyma distal to the tumor. The remaining
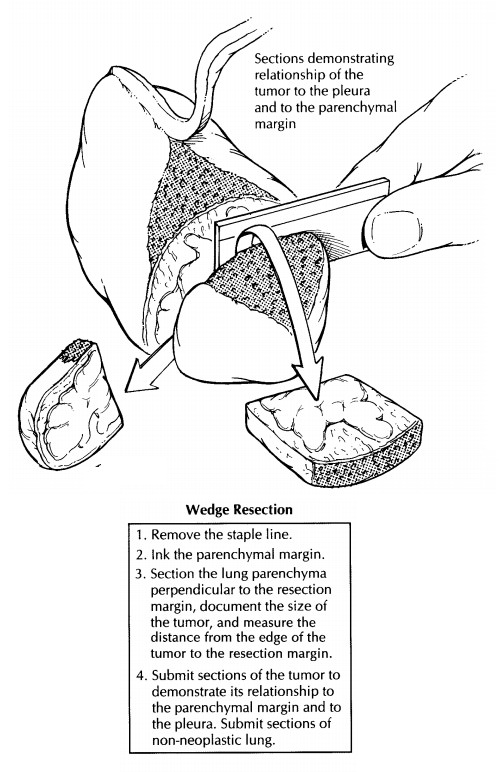
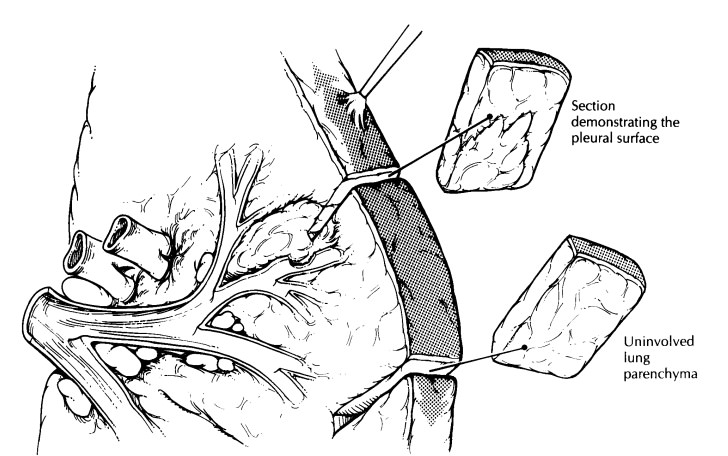
lung parenchyma can then be sec-tioned at 1-cm intervals. For peripherally
located tumors, a site of origin from an airway may not be apparent. In these
instances, serial sections through the tumor perpendicular to the closest
segmental bronchus may best reveal the relation-ships of the tumor to the
pleura, to the surround-ing lung parenchyma, and to the small airways.
For
non-neoplastic lung diseases, section the specimen in a manner that best
correlates with the radiographic studies. For example, thin serial sections of
the fixed specimen in the transverse plane can be used to arrive at a
one-to-one cor-relation between changes identified in computed tomography scans
and the pathology. In the de-scription of these large lung specimens, do not
lose sight of the systematic approach that in-cludes descriptions of all five
basic components of the lung.
For
specimens that harbor a neoplasm, the major aims of tissue sampling for
histology are to document the tumor type, the origin of the tumor, the extent
of the tumor (local and metastatic), and the adequacy of tumor resection. To
assess tumor type, submit four sections of tumor, both from the center of the
tumor and from the inter-face of the tumor with the surrounding lung tissue.
Make every effort to demonstrate the rela-tionship of the tumor to an
associated airway. For more proximal tumors with an apparent en-dobronchial
component, take sections along the involved airway to include both tumor and
bron-chus. For peripheral lesions, a site of origin from a small airway may not
be apparent. In these cases, take sections through the tumor in a plane
perpendicular to the airways. Document tumor extension to or through the pleura
with sections taken at right angles to the pleura in areas of retraction.
Similarly, take sections of tumor extension into the pulmonary vessels, hilar
soft tissues, and chest wall. Submit all lymph nodes identified in the hilar
and peribronchial regions. If the specimen also contains a portion of chest
wall, take sections and margins from all of the attached structures (parietal
pleura, skin, soft tissues, and ribs), as if this block were its own specimen.
Finally, submit sections of non-neoplastic lung from each lobe, including
sections taken distal to the tumor for documentation of an obstructive
pneumonic process.
For
diffuse non-neoplastic processes, submit representative sections of lung
parenchyma from each lobe as well as sections of proximal airways. If a focal
lesion is encountered, section it in the manner described above for a neoplasm.
Related Topics