Chapter: Clinical Dermatology: Diagnosis of skin disorders
Keratosis follicularis (DarierŌĆÖs disease)
Keratosis follicularis (DarierŌĆÖs
disease)
Cause
This
rare condition is inherited as an autosomal dominant trait. Fertility tends to
be low and many cases represent new mutations. The abnormal gene (on chromosome
12q23-q24.1) encodes for a molecule important in a signalling pathway that
regulates cellŌĆō cell adhesion in the epidermis.
Presentation
The
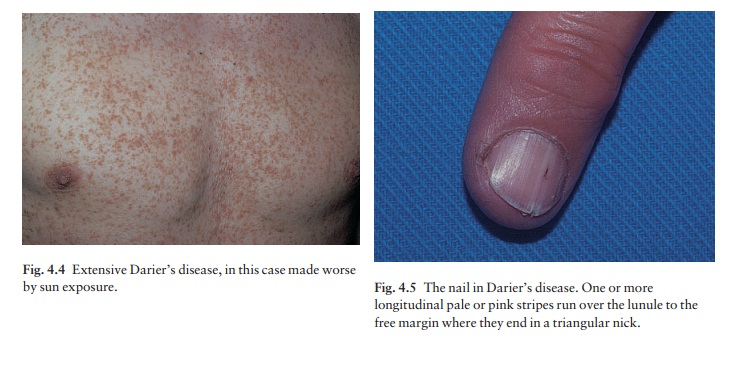
first signs usually appear in the mid-teens, some-times after overexposure to
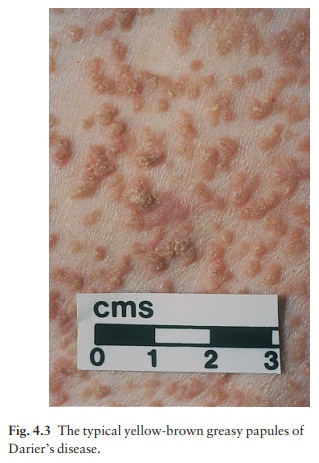
sunlight. The characteristic lesions are small pink or brownish papules with a
greasy scale (Fig. 4.3). These coalesce into warty plaques in a ŌĆśseborrhoeicŌĆÖ
distribution (Fig. 4.4). Early lesions are often seen on the sternal and
interscapular areas, and behind the ears. The severity of the condition varies
greatly from person to person: sometimes the skin is widely affected. The
abnormalities remain for life, often causing much embarrassment and discomfort.
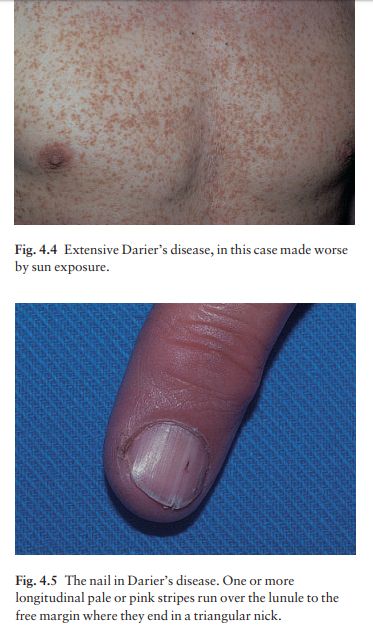
Other changes include lesions looking like plane warts on the backs of the hands, punctate keratoses or pits on the palms and soles, cobblestone-like changes in the mouth, and a distinctive nail dystrophy in which white or pinkish lines or ridges run longitudinally to the free edge of the nail where they end in triangular nicks (Fig. 4.5).
Complications
Some
patients are stunted. Personality disorders, including antisocial behaviour,
are seen more often than would be expected by chance. An impairment of delayed
hypersensitivity may be the basis for a tendency to develop widespread herpes
simplex and bacterial infections. Bacterial overgrowth is respons-ible for the
unpleasant smell of some severely affected patients.
Differential diagnosis
The
distribution of the lesions may be similar to that of seborrhoeic eczema, but
this lacks the warty papules of DarierŌĆÖs disease. The distribution differs from
that of acanthosis nigricans (mainly flexural) and of keratosis pilaris
(favours the outer upper arms and thighs). Other forms of folliculitis and
GroverŌĆÖs disease can also cause
confusion.
Investigations
The
diagnosis should be confirmed by a skin biopsy, which will show characteristic
clefts in the epidermis, and dyskeratotic cells.
Treatment
Severe
and disabling disease can be dramatically allevi-ated by long-term acitretin.
Milder cases need only topical keratolytics, such as salicylic acid, and the
control of local infection.
Related Topics