Chapter: Clinical Dermatology: Diagnosis of skin disorders
Keratoderma of the palms and soles
Keratoderma
of the palms and soles
Inherited types
Many
genodermatoses share keratoderma of the palms and soles as their main feature;
they are not described in detail here. The clinical patterns and modes of
inher-itance vary from family to family. Punctate, striate, diffuse and
mutilating varieties have been documented, sometimes in association with
metabolic disorders such as tyrosinaemia, or with changes elsewhere. The
punctate type is caused by mutations in the keratin 16 gene on chromosome
17q12-q21; the epidermolytic type by mutations in the gene for keratin 9, found
only on palms and soles.
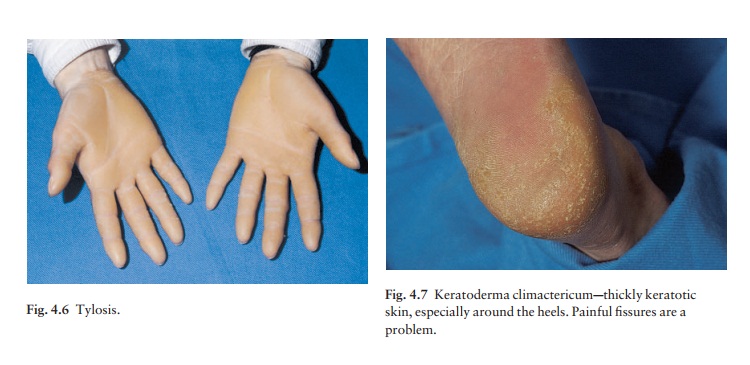
The
most common pattern is a diffuse one, known also as tylosis (Fig. 4.6), which
is inherited as an autosomal dominant trait. In a few families these changes
have been associated with carcinoma of the oesophagus, but in most families
this is not the case.
Treatment
tends to be unsatisfactory, but keratolytics such as salicylic acid and urea
can be used in higher concentrations on the palms and soles than elsewhere.
Acquired types
It
is not uncommon for normal people to have a few inconspicuous punctate
keratoses on their palms, and it is no longer thought that these relate to
inter-nal malignancy, although palmar keratoses caused by arsenic may have this
association. Black patients are prone to keratotic papules along their palmar
creases.
Keratoderma
of the palms and soles may be part of the picture of some generalized skin
diseases such as pityriasis rubra pilaris
and lichen planus.
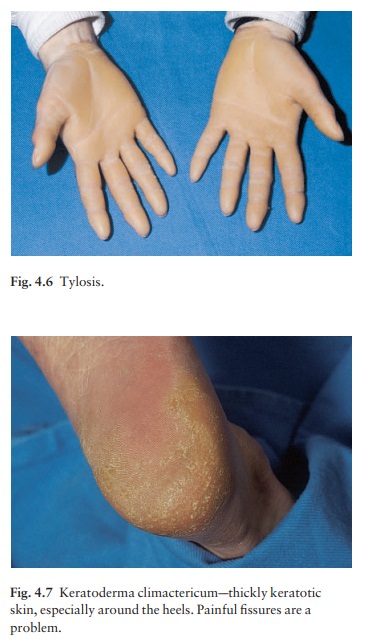
A
distinctive pattern (keratoderma climactericum) is sometimes seen in
middle-aged women at about the time of the menopause. It is most marked around
the borders of the heels where painful fissures form and interfere with walking
(Fig. 4.7). Regular paring and the use of keratolytic ointments are often more
help-ful than attempts at hormone replacement, and the condition tends to
settle over a few years. Acitretin in low doses may be worth a trial.
Related Topics