Chapter: Essentials of Psychiatry: Hypnosis
Hypnotizability Scales
Hypnotizability
Scales
Hypnotizability
scales have been developed for clinical use (Hypnotic Induction Profile
[Spiegel and Spiegel, 1978]; Stan-ford Hypnotic Clinical Scale [Hilgard and
Hilgard, 1975]). These scales are designed for comfortable use even with
patients who have severe psychiatric disturbances (Spiegel and Spiegel, 1978;
Spiegel et al., 1982, 1988). They are
well accepted by patients and help to bypass anxiety by shifting the focus of
the interaction from one in which the therapist tries to make the patient have
a hypnotic experience to one in which the therapist assesses the patient’s
response to a set of instructions, like any other medical or psychological test
(Spiegel and Spiegel, 1978). The therapist focuses on evaluating the patient’s
ability to enter the state rather than on getting the person into the state.
They all involve a struc-tured hypnotic induction and an assessment of the
subject’s re-sponse to a variety of instructions, such as alterations in the
sense of control over body movements, physical sensations, orientation to time
and space, and perception. Furthermore, such a standard-ized testing induction
permits an important deduction regarding the hypnotic capacity of the subject.
The restricted range of in-put from the therapist maximizes the information
provided by variations in subjects’ responses. After the results of the testing
are discussed with the subject, both can proceed knowledgeably, choosing to use
hypnosis or other techniques in the service of an agreed on treatment goal.
The use
of this kind of objective measurement has several clinical advantages and
therapeutic implications (Table 72.3).
Hypnosis Induction Profile
The
Hypnotic Induction Profile (Figure 72.1) is a useful clini-cal screening test
for hypnotic capacity. It consists of a number
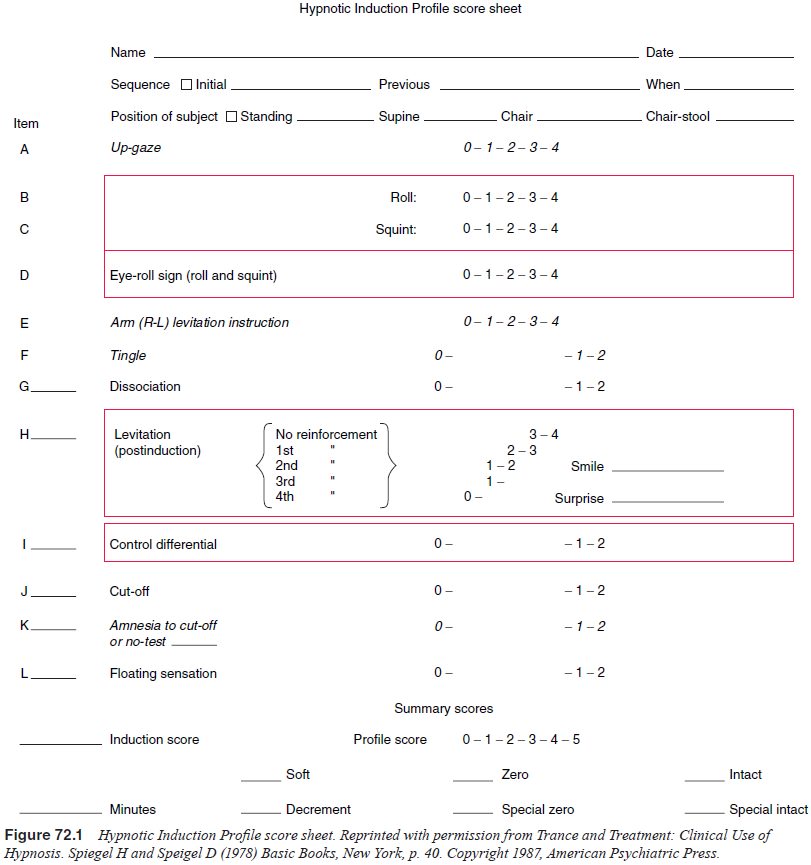
of the
simple instructions that allow the measurement of pa-tients’ natural ability to
tap into and use their hypnotic capac-ity. It begins with a simple and quick
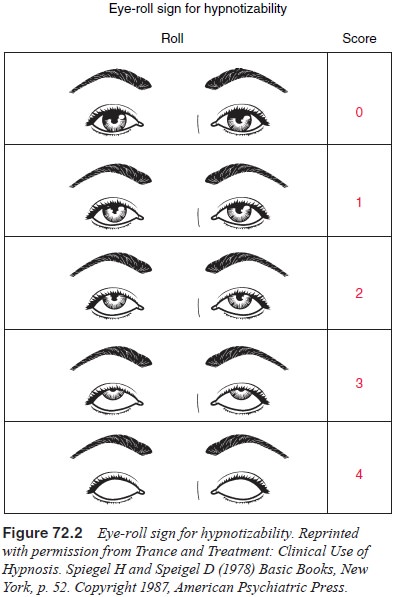
induction, counting from 1 to 3, accompanied by the eye roll. This involves
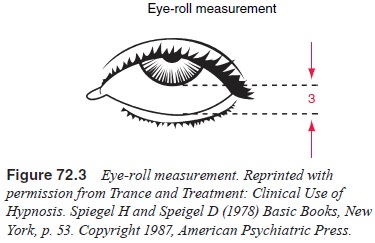
instructed upward gaze and lowering of the eyelids (Figure 72.2). The
dis-sociation between upward gaze and lowering of the eyelid can be scored
(Figure 72.3), providing the therapist with an initial prediction of the
subject’s hypnotic capacity. The eye roll is then followed by a series of
instructions briefly to influence the subject’s behavior during and shortly
after the test (posthyp-notic suggestions). The Hypnotic Induction Profile
allows the therapist to rate the subject on five items (Table 72.4) assess-ing
cognitive and behavioral aspects of the single continuous but brief hypnotic
experience elicited during the test. These
are: 1)
ability to experience a sense of dissociation of the left hand from the rest of
the body; 2) hand levitation, or floating of the hand back up in the air after
being pulled down; 3) sense of involuntariness or unconscious compliance while
elevating the hand; 4) response to the cutoff signal ending the hypnotic
experience; and 5) sensory alteration in the hand or elsewhere in the body.
Scores on the Hypnotic Induction Profile are significantly but moderately correlated with those on the Stanford scales (Orne et al., 1979) and provide useful discrimination among different psychiatric disorders, as described in the following section.
Related Topics