Chapter: Medicine and surgery: Nutritional and metabolic disorders
Hyperlipidaemia
Hyperlipidaemia
Definition
Increased concentration of specific lipoproteins in the plasma. Although ‘normal’ reference ranges exist even within this range, there is still a risk of developing complications.
Aetiology/pathophysiology
Lipids are found in dietary fat and are an important energy source as well as provide essential vitamins and fatty acids. The two main lipids are triglycerides and cholesterol, which are found in dietary fat and may also be synthesised in the liver and adipose tissue (see Fig. 13.1).
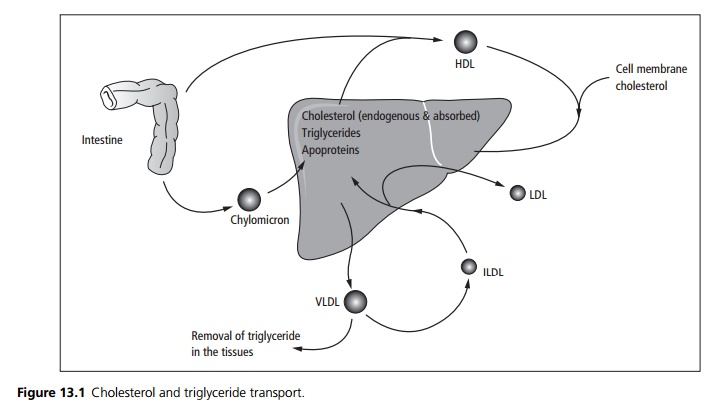
· Lipids are insoluble; they are absorbed from the small intestine as chylomicrons (a combination of triglyceride, cholesterol and apoproteins). These are then transported to the liver where the triglyceride is removed and the remaining cholesterol-containing particle is also taken up by the liver.
· The liver synthesises very-low-density lipoproteins (VLDL), containing lipoproteins, triglyceride and cholesterol, these circulate allowing trigyceride to be removed and utilised. The end product, deplete of triglyceride, is termed an intermediate-density lipoprotein (IDL).
· Most of these are broken down in the liver. Some are further depleted of triglyceride and are released as low-density lipoproteins (LDL) – the main cholesterol carrier.
· High-density lipoproteins (HDL) from the intestine and the liver collect cholesterol from cell membranes in the tissue and transport it back to the liver.
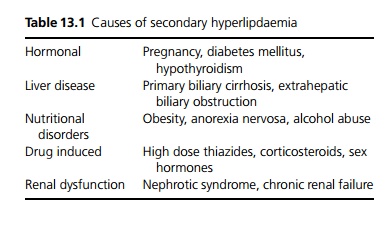
Hyperlipidaemias are classified as primary and secondary (see Table 13.1).
Primary hyperlipidaemia is a group of inherited conditions subdivided into those that cause hypertriglyceridaemia, hypercholesterolaemia and combined hyperlipidaemia.
· Hypertriglyceridaemia: Familial hypertriglyceridaemia, lipoprotein lipase deficiency, apoprotein C-II deficiency.
· Hypercholesterolaemia: Heterozygous familial hyper-cholestrolaemia (LDL receptor deficiency), homozygous familial hypercholesterolaemia, defects in apo-protein B.
· Combined hyperlipidaemia: Familial combined hyperlipidaemia, remnant hyperlipidaemia.
Clinical features
The clinical signs of hypercholesterolaemia are premature corneal arcus, xanthelasmata and tendon xanthomata. Acute pancreatitis and eruptive xanthomata are features of hypertriglyceridaemia. More commonly it is diagnosed through targeted screening of high-risk patients (family history of hyperlipidaemia or coronary heart disease, hypertensive, diabetic and obese patients.
Complications
Atherosclerosis leads to coronary heart disease, cerebrovascular disease and peripheral vascular disease. Hypertriglyceridaemia can cause acute pancreatitis.
Investigations
Random, non-fasting plasma cholesterol is used as a screen in low-risk populations. Full fasting lipid profile, including total, LDL and HDL cholesterol and triglyceride, is used if high cholesterol is found or in high-risk patients.
Management
The management of hyperlipidaemia is based on an assessment of overall cardiovascular risk and current cardiovascular status.
General measures include weight loss, lipid-lowering diets, reduction of alcohol intake, stopping smoking and increasing exercise.
Control of hypertension is important preferably avoiding drugs that raise lipid or glucose levels.
Lipid-lowering drugs include the following:
1. Cholesterol-lowering drugs include resins, which sequestrate bile salts such as cholestyramine.
2. Cholesterol and triglyceride lowering drugs such as HMG CoA reductase inhibitors (statins), fibrates, nicotinic acid and analogues.
3. Triglyceride-lowering drugs such as fish oils (omega-3 marine triglycerides) may be required.
Related Topics