Chapter: Essentials of Psychiatry: Anxiety Disorders: Generalized Anxiety Disorder
Generalized Anxiety Disorder: Differential Diagnosis
Differential Diagnosis
Psychiatric Conditions
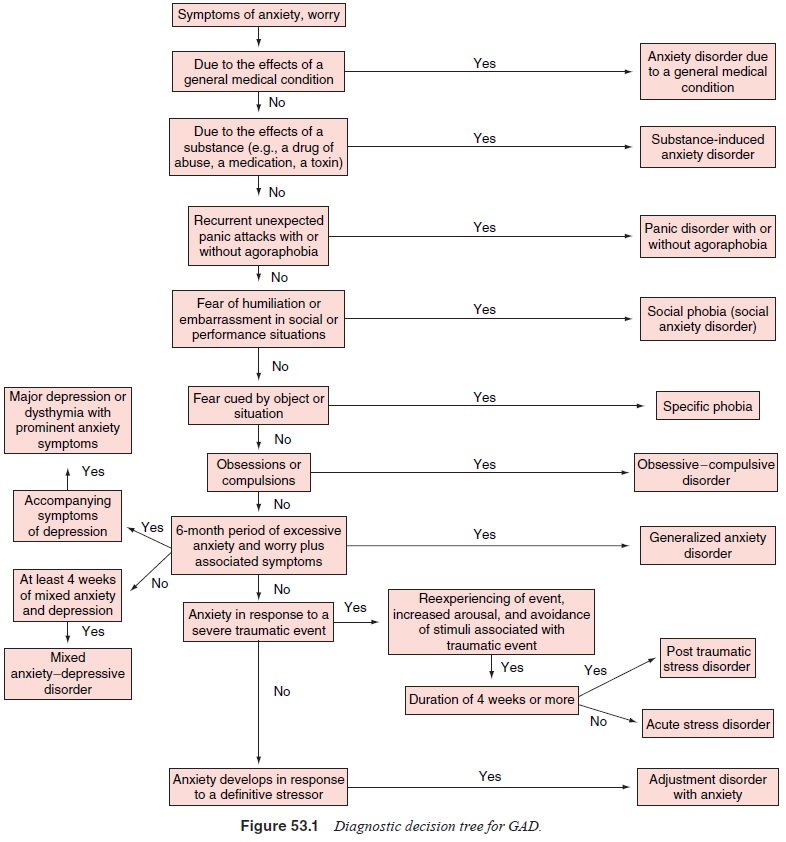
GAD and other psychiatric disorders such as major depressive disorder,
often creates diagnostic and treatment dilemmas for the clinician and may
complicate the difficult task of differential di-agnosis and treatment
planning. This section will highlight the major disorders that should be
considered in the differential di-agnosis of GAD (Figure 53.1).
Major Depressive Disorder and Dysthymic Disorder
Several symptom profiles discriminate between major depres-sive disorder
or dysthymic disorder and GAD. Patients with ma-jor depressive disorder exhibit
higher rates of dysphoric mood, psychomotor retardation, suicidal ideation,
guilt, hopelessness and helplessness, as well as more work impairment than
patients with GAD. In contrast, patients with GAD show higher rates of somatic
symptoms, specifically, muscle tension and autonomic symptoms (e.g.,
respiratory or cardiac complaints) than depressed patients.
Panic Disorder With/Without Agoraphobia
Some researchers have suggested that GAD is attributable to panic disorder.
However, clear differences exist between GAD and panic disorder. For example,
panic disorder is characterized by the presence of panic attacks; that is,
recurrent, discrete epi-sodes of intense anxiety or fear associated with a
cluster of so-matic symptoms reflecting autonomic hyperactivity such as rapid
heartbeat, dizziness, numbness or tingling, trouble breathing or choking, and
nausea or vomiting. In contrast, patients with GAD experience predominantly
symptoms of muscle tension and vigi-lance such as fatigue, muscle soreness,
insomnia, difficulty con-centrating, restlessness and irritability. Patients
with panic disor-der tend to seek treatment earlier in life than patients with
GAD. Additionally, reports of types of worry differ between those diagnosed
with GAD and those with panic disorder. For exam-ple, panic patients worry
about having additional panic attacks, whereas GAD patients worry
unrealistically about a number of everyday issues.
Obsessive–Compulsive Disorder
Anxiety is part of the clinical picture of obsessive–compulsive disorder
(OCD) and may be a central factor in initiating and main-taining obsessions and
compulsions. Interestingly there are also some data suggesting that OCD and GAD
may be related. For ex-ample, Black and associates (1992) found an increased
prevalence of GAD among relatives of patients with OCD. However, several
features distinguish the excessive worry that accompanies GAD from the
obsessional thoughts of OCD. Obsessive thoughts are described as ego-dystonic intrusions
that often take the form of urges, impulses, or images. They are often
senseless and are fre-quently accompanied by time-consuming compulsions
designed to reduce mounting anxiety. In contrast, the worries in GAD are about
realistic concerns, such as health and finances.
Other Anxiety Disorders
In phobic disorders, the anxiety is characteristically associ-ated with
a specific phobic object or situation that is frequently avoided by the
patient. Such is the case with social anxiety dis-order as well, in which the
individual is afraid of or avoids situ-ations in which he or she may be the
focus of potential scrutiny by others. Anxiety is also a characteristic part of
the presentation of post traumatic stress disorder (PTSD) and acute stress
disor-der. However, unlike in GAD, the principal symptoms experi-enced in PTSD
and acute stress disorder follow exposure to a traumatic event and are
characterized by avoidance of reminders of the event and persistent
reexperiencing of the traumatic event. In addition, in contrast to GAD which
must last at least 6 months, acute stress disorder does not persist for more
than 4 weeks. Finally, in adjustment disorders anxiety when present occurs in
response to a specific life stressor or stressors and generally does not
persist for more than 6 months (American Psychiatric Association, 1994).
Normal Anxiety
Worry and anxiety are part of normal human behavior, and it may be
difficult to define a cutoff point distinguishing normal or trait anxiety
(i.e., a relatively stable tendency to perceive various situations as
threatening) from GAD. However, in-dividuals suffering from a “disorder”
exhibit significant dis-tress and impairment in functioning as a result of
their anxiety symptoms.
Anxiety Disorder due to a General Medical Condition
Many general medical conditions may present with prominent anxiety
symptoms. If not identified and properly addressed, these conditions may
adversely affect the treatment outcome of the anxious patient. In this section
we will highlight important medical conditions in the differential diagnosis of
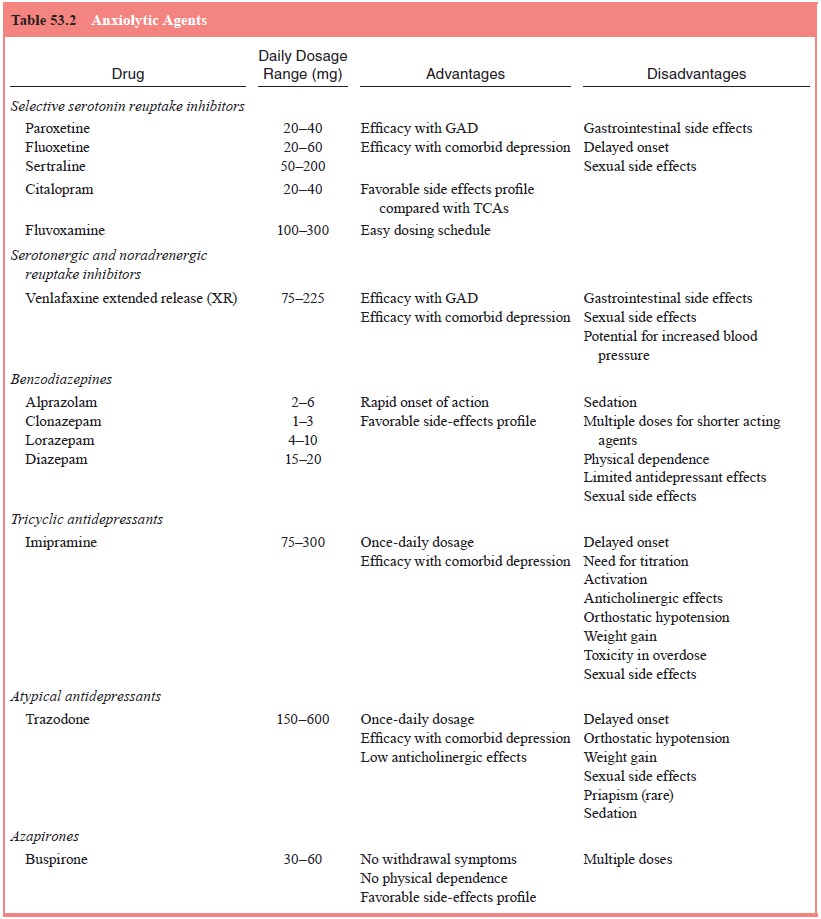
generalized anxiety (see Table 53.2).
Cardiovascular Disorders
Patients with GAD may complain of palpitations, skipped heart-beats and
chest pain. In addition, many GAD patients, espe-cially males, fear having an
acute myocardial infarction and often present to the emergency room for
evaluation. However, most patients with GAD without a concomitant
cardiovascular disease do not experience severe chest pain. Following the
con-troversial evidence suggesting an association between mitral valve prolapse
(MVP) and panic disorder, researchers evalu-ated the prevalence of MVP in
patients with GAD and found no evidence of increased prevalence in patients
with GAD. Nevertheless, patients with anxiety symptoms associated with
unexplained chest pain should be evaluated for possible cardio-vascular
disease.
Hyperthyroidism
Anxiety
is a prominent feature of hyperthyroidism with some overlap in the
symptomatology of thyrotoxicosis and GAD. Symp-toms such as tachycardia,
tremulousness, irritability, weakness and fatigue are common to both disorders.
In GAD, however, the peripheral manifestations of excessive concentrations of
circulat-ing thyroid hormones are absent, including symptoms such as weight
loss, increased appetite, warm and moist skin, heat intol-erance and dyspnea on
effort. Presence of goiter makes the diag-nosis of hyperthyroidism likely;
however, the absence of thyroid enlargement does not exclude it. Thus,
confirmatory laboratory tests (free T4, T3 and TSH) assume significant diagnostic impor-tance. In mild cases,
laboratory tests may be within the upper limit of the normal range, in which
case a thyroid releasing hor-mone stimulation test is indicated.
Pheochromocytomas
Pheochromocytomas, also known as chromaffin tumors, pro-duce, store and
secrete catecholamines. They are derived most often from the adrenal medulla,
as well as the sympathetic ganglia and occasionally from other sites. The
clinical fea-tures of these tumors, most commonly hypertension and
hy-pertensive paroxysms, are predominantly due to the release of
catecholamines. Patients may also experience diaphoresis, tachycardia, chest
pain, flushing, nausea and vomiting, head-ache and significant apprehension.
Although the clinical pres-entation frequently mimics spontaneous panic
attacks, pheo-chromocytomas should also be considered in the differential
diagnosis of GAD. The diagnosis of pheochromocytoma can be confirmed by
increased levels of catecholamines (epine-phrine and norepinephrine) or
catecholamine metabolites (metanephrines and vanillylmandelic acid) in a
24-hour urine collection.
Other Medical Conditions
Menopause is commonly referred to as the period that encom-passes the
transition between the reproductive years and beyond the last episode of
menstrual bleeding. Frequently associated with significant anxiety, menopause
should be considered in the differential diagnosis of GAD. However, other
associated symptoms such as vasomotor instability, atrophy of urogenital epithelium
and skin, and osteoporosis make the diagnosis of menopause probable. Another
endocrinologic disorder, hyper-parathyroidism, can present with anxiety
symptoms, and the ini-tial evaluation of serum calcium levels may be indicated.
Finally, certain neurologic conditions such as complex partial seizures,
intracranial tumors and strokes, and cerebral ischemic attacks may be
associated with symptoms typically observed in anxiety disorders and may
require appropriate evaluation.
Substance-induced Anxiety Disorder
Anxiety disorders can occur frequently in association with in-toxication
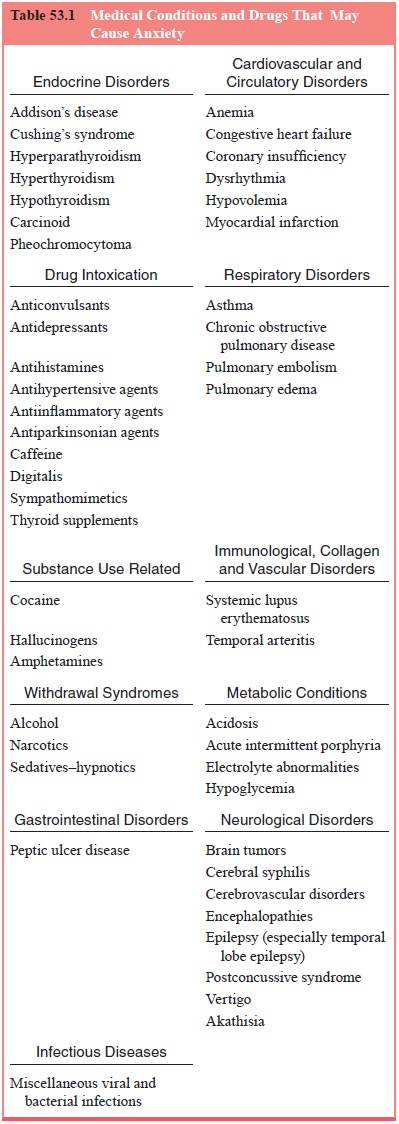
and withdrawal from several classes of substances (see Table 53.1). Excessive
use of caffeine, especially in children and adolescents, may cause significant
anxiety. Cocaine intoxi-cation may be associated with anxiety, agitation and
hypervigi-lance. During cocaine withdrawal, patients may also present with
prominent anxiety, irritability, insomnia, fatigue, depression and cocaine
craving. Adverse reaction to marijuana includes extreme anxiety that usually
lasts less than 24 hours. Mild opioid with-drawal presents with symptoms of
anxiety and dysphoria. How-ever, accompanying symptoms such as elevated blood
pressure, tachycardia, pupilary dilatation, rhinorrhea, piloerection and lac-rimation
are rare in patients with GAD.
The clinical phenomenology observed both in alcohol and
sedative–hypnotic drug withdrawal and in GAD, although variable, may be highly
similar. In both conditions, nervousness, tachycardia, tremulousness, sweating,
nausea and hyperventila-tion occur prominently. Additionally, the same drugs
(i.e., ben-zodiazepines) can be used to treat anxiety symptoms, and some
patients may use alcohol in an attempt to alleviate anxiety. Thus, the symptoms
of an underlying anxiety disorder may be difficult to differentiate from the
withdrawal symptoms associated with the use of benzodiazepines or alcohol.
The use
of many commonly prescribed medications may produce side effects manifesting as
anxiety (see Table 53.1). Such medications include sympathomimetics or other
bronchodilators such as theophilline, anticholinergics, antiparkinsonian
prepara-tions, corticosteroids, thyroid supplements, oral contraceptives, The
use of many commonly prescribed medications may produce side effects
manifesting as anxiety (see Table 53.1). Such medications include
sympathomimetics or other bronchodilators such as theophilline,
anticholinergics, antiparkinsonian prepara-tions, corticosteroids, thyroid
supplements, oral contraceptives,
Related Topics