Chapter: Basic Radiology : Radiology of the Breast
Exercise: The Follow-Up Mammogram(The Asymptomatic Patient)
EXERCISE 5-5. THE FOLLOW-UP MAMMOGRAM
5-14. Which of the
following statements about Case 5-14 is false (Figure 5-24)?
A.
The abnormal finding is a spiculated mass.
B.
The rate of change is too slow for a breast cancer.
C.
A malpractice claim should not be encouraged.
D.
The lesion is probably not palpable.
E.
This change warrants biopsy.
5-15. With respect to the
calcifications in Case 5-15 (Figure5-25), which statement is false?
A.
They may be described as pleomorphic.
B.
The coarse nature of some of the calcifications suggests this is
a benign process.
C.
They signal an aggressive malignancy.
D.
They are most likely due to necrosis in duct walls.
E.
Magnification should be performed to assess the extent of
disease.
5-16. With respect to the
calcifications in Case 5-16 (Figure5-26), which statement is true?
A.
They may be described as granular.
B.
The regional distribution makes them highly sus-picious.
C.
Follow-up alone would be inadequate.
D.
The new onset indicates a high probability of ma-lignancy.
E.
They have a less than 20% chance of being malig-nant.
Radiologic Findings
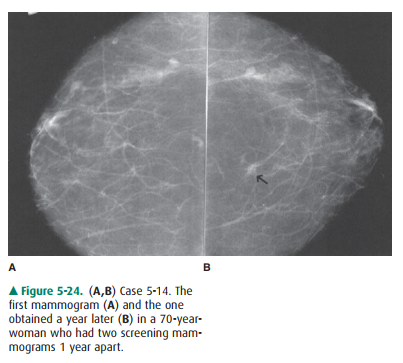
5-14. This case shows
back-to-back craniocaudal views of the right breast obtained 1 year apart. In
the interval, a small spiculated mass has enlarged so as to become more
apparent (arrow) (B is the correct answer to Question 5-14).
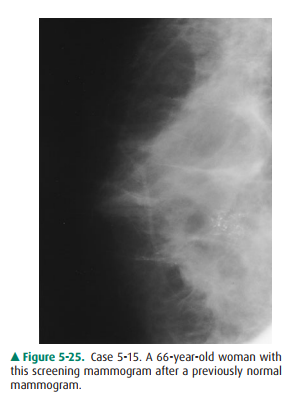
5-15. The mammogram of
the patient in this case shows a cluster of microcalcifications posteriorly in
the central aspect of the breast. Previous mammograms have been normal (B is
the correct answer to Question 5-15).
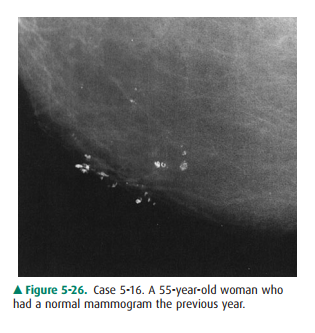
5-16. Magnification view
of a portion of the breast of the patient in this case shows coarse
calcifications, some of which are rounded or ringlike (E is the correct an-swer
to Question 5-16).
Discussion
Case 5-14 illustrates the concept of developing density. A
de-veloping density is any opacity that increases in size or density over time.
All such opacities should be evaluated critically, as they can be signs of
carcinoma. This concept is based on the natural behavior of breast cancer,
which generally grows slowly. With periodic screening, the early tumor will be
imaged but unrecognized on early images and may not be detected until 1, 2, 3,
or more years later. Tumors 5 mm or smaller are very difficult to differentiate
from normal breast tissue, but masses larger than 1 cm are more easily
detected. The typical breast cancer has been present for several years by the
time it is 1 cm in size. Therefore, breast cancers are routinely visible in
retrospect on previous mammograms if the patient has had frequent screening.
This does not mean, however, that mal-practice has occurred. If the cancer is
still small, no harm has been done and more harm could potentially be done by
biop-sying all such tiny densities, because most of them would be normal breast
(Statement C is true). Being suspicious but judi-cious with any developing
density, therefore, is necessary to de-tect breast cancer early without
unnecessary biopsy.
This patient has a small (about 1 cm) spiculated mass in the
central part of the breast (Statement A is true). It has in-creased slightly in
size over 1 year, with a growth rate typical for breast carcinoma (Statement B
is false and is the correct answer to Question 5-14). Being so small in a
medium-sized breast, it is unlikely to be palpable (Statement D is true) and,
therefore, would require imaging guidance for any biopsy. The spiculated
margins, the rate of growth, and the patient’s age group all make this a very
suspicious lesion, and biopsy is warranted (Statement E is true). This lesion
was an infiltrat-ing ductal carcinoma.
Case 5-15 illustrates a new finding after a previous normal
screening. There is a cluster of microcalcifications in the cen-tral area. Note
that the calcifications are small and irregular, but we do not see their
configuration exquisitely; nor can we be confident of the extent of disease,
because there may be other smaller calcifications that we do not see. The
patient, therefore, requires recall for magnification mammography (Figure 5-27)
(Statement E is true). On magnification, we can appreciate that the
calcifications are of many different sizes and shapes (ie, pleomorphic)
(Statement A is true). Malig-nant microcalcifications are usually less than 0.5
mm in size, and the very coarse calcifications are classically benign.
How-ever, there is significant overlap, and configuration is gener-ally a more
helpful sign. Malignant calcifications are usually either granular or linear
and branching.
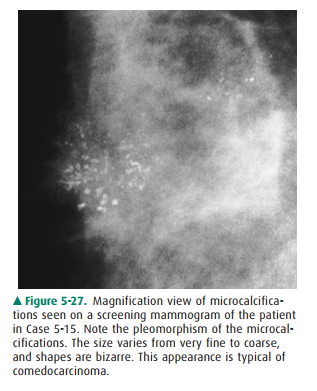
These granular, linear, and branching calcifications are typical
of intraductal carcinoma. The aggressive type of in-traductal carcinoma, comedo
or high-nuclear-grade carci-noma, causes necrosis in the cancerous mammary duct
walls. Calcifications form in areas of necrosis, forming a “cast” of the duct.
This process results in the linear and branching forms of calcification
(Statements C and D are true). Patho-logic analysis of this tissue showed
intraductal carcinoma of the comedo type.
Lesser degrees of necrosis result in smaller, more granular
calcifications, whereas extensive necrosis yields rather large rod-shaped or
branched calcifications. Option B is false be-cause, although large
calcifications alone are usually benign, the mixture of tiny irregular
calcifications with the coarse casting calcifications remains very suspicious
for malignancy.
In Case 5-16, the mammogram detail shows typical be-nign
calcifications. Benign calcifications take many forms, but if we see rings with
lucent centers, as in this case, we can rest assured that they are benign.
These rings are calcifying microcystic areas of fat necrosis. This is a very
common be-nign finding. Punctate, or dotlike, calcifications are also usu-ally
benign if uniform and smooth. Granular calcifications are more angular, like
broken needle tips, and would be more suspicious (Statement A is false).
Benign calcifying processes such as fibroadenoma, scleros-ing
adenosis, and fat necrosis can all be unifocal, or regional, as well as
multifocal or diffuse; therefore, distribution alone does not make
calcifications suspicious (Statement B is false).
Benign processes of many types do present in adulthood and
therefore may appear de novo after a previously normal screening examination.
Again, the configuration of calcifica-tions is more helpful (Statement D is
false).
For obviously benign calcifications such as these, routine
follow-up alone is adequate (Statement C is false). Some cal-cifications are
obviously malignant as in Case 5-15. A third group of calcifications is
classified as indeterminate, and these require further evaluation, either close
mammo-graphic follow-up or some type of biopsy. Taken as a group, biopsied
microcalcifications historically have had a rate of malignancy of only 20%.
Therefore, Option E is true, be-cause these ringlike calcifications have a
better-than-average chance of being benign.
Related Topics