Chapter: Basic Radiology : Radiology of the Breast
Exercise: Architectural Distortion and Asymmetric Density(The Asymptomatic Patient)
EXERCISE 5-4.
ARCHITECTURAL DISTORTION AND ASYMMETRIC DENSITY
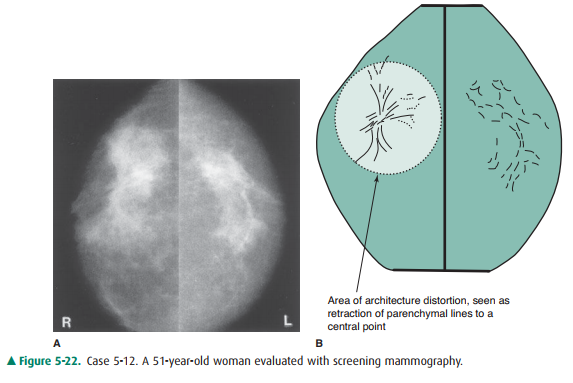
5-12. Concerning the
architectural distortion in the right breast in Case 5-12 (Figure 5-22), which
statement is false?
A.
Without history of biopsy, scarring is unlikely.
B.
Previous mammograms could be very helpful.
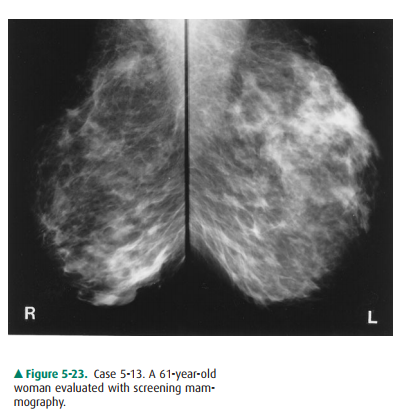
5-13. The mammographic appearance in
Case 5-13 (Figure5-23) is least likely to be caused by normal breasts,postsurgical
change.,trauma, cystic disease,tumor.
Radiologic Findings
5-12.Bilateral craniocaudal views show architecture dis-tortion in
the right breast without a discrete domi-nant mass (C is the correct answer to
Question 5-12).
5-13.Bilateral mediolateral oblique views of patient in thiscase show
areas of asymmetric density in the left upper and right lower breast. The
densities are inter-spersed with fat. Margins are generally concave, and there
is no architectural distortion (D is the correct answer to Question 5-13).
Discussion
Although normal breast tissue is
remarkably symmetric, it is never exactly the same on both sides. The challenge
in mam-mography is to recognize normal variation and to be able to distinguish
nonpathologic asymmetry from disease. This is not always possible, particularly
in the asymptomatic group. A high index of suspicion is needed in evaluating
the screen-ing mammogram, just as in the baseline clinical breast exam-ination.
Once asymmetry is noted mammographically, a careful, focused breast examination
is needed. If no suspi-cious areas are detected and if the radiographic
features sug-gest fibroglandular tissue, then follow-up alone is adequate.
Radiographically, we look for a homogeneous, nondistorted pattern of fat
interspersed with lobular densities. Any domi-nant mass or architectural distortion
should cause concern.
In Case 5-12, one area shows a
different architectural pat-tern. The lines of tension appear to pull to a
central focus. This is a classic appearance of invasive lobular carcinoma.
Remember that 90% of the breast cancers are ductal in ori-gin, and the other
10% are lobular, as in this case. This type of carcinoma shows a subtle
infiltrating pattern much more often than does ductal carcinoma (Statement D is
true).
One of the problems with this
disease is that it is difficult to describe the extent of tumor
mammographically. There is a large area of asymmetric architecture in this
patient, but where the tumor ends is unclear. This patient had a carci-noma
that measured 4 cm.
A correlated clinical examination
often reveals abnormal-ities not detected without the guidance of mammographic
findings (Statement C is false). Biopsy of any suspicious-feeling area is
strongly recommended. Studies have shown that a high percentage of carcinomas
“missed” at mammog-raphy appear as architecture distortion or asymmetric
den-sity. This patient did have a large area of thickening in the upper aspect
of this breast, confirming the suspicious nature of the mammographic findings.
Previous mammograms are
definitely useful in evaluating architecture distortion and asymmetric density.
If the finding is unchanged over time, no further action may be needed. If the
finding is new or is increasing, it is more easy to recognize (Statement B is
true). Hormonal therapy may indeed have an asymmetric effect (Statement E is
true), but it does not take the form of architecture distortion.
Surgical biopsy may result in
such distortion of the archi-tecture, but precise correlation with location and
timing of the surgery is needed (Statement A is true).
Unlike the previous patient, the
woman in Case 5-13 has multiple areas of breast asymmetric density. There is a
large area in the upper part of the left breast and a smaller area in the lower
part of the right breast. Both areas show fat inter-spersed with fibroglandular
densities. There is no architec-tural distortion. Margins of the larger
opacities are generally concave—a sign of benignity. There are no dominant or
cir-cumscribed masses, and cystic disease therefore would not be part of the
differential diagnosis, because cysts are rounded masses. Having learned from
the previous case that missed carcinoma often presents as asymmetric density,
tumor must remain in the differential diagnosis, and answer E is incorrect.
Both trauma and postoperative
change can lead to ill-defined asymmetric density. With trauma there may be
bleeding, contusion, or actual deformity, if severe. With sur-gery, asymmetry
results both from removal of normal tis-sues, leaving less density on the
operated side, and from surgical trauma (hematoma and distortion), which causes
increased localized densities. Therefore, options B and C are both incorrect.
The most likely cause of this woman’s mam-mographic appearance is normal breast
tissue, and answer A is incorrect. The multiplicity and bilaterality of areas
of asymmetry, the lack of signs or symptoms of breast cancer, and the
fibroglandular characteristics of the densities all support this diagnosis.
Related Topics