Chapter: Basic & Clinical Pharmacology : Drugs of Abuse
Drugs that Bind to Transporters of Biogenic Amines
DRUGS THAT BIND TO TRANSPORTERS
OF BIOGENIC AMINES
Cocaine
The
prevalence of cocaine abuse has increased greatly over the last decade and now
represents a major public health problem world-wide. Cocaine is highly
addictive (relative risk = 5), and its use is associated with a number of
complications.
Cocaine
is an alkaloid found in the leaves of Erythroxylon
coca, a shrub indigenous to the Andes. For more than 100 years, it has been
extracted and used in clinical medicine, mainly as a local anesthetic and to
dilate pupils in ophthalmology. Sigmund Freud famously proposed its use to
treat depression and alcohol depen-dence, but addiction quickly brought an end
to this idea.
Cocaine
hydrochloride is a water-soluble salt that can be injected or absorbed by any
mucosal membrane (eg, nasal snort-ing). When heated in an alkaline solution, it
is transformed into the free base, “crack cocaine,” which can then be smoked.
Inhaled crack cocaine is rapidly absorbed in the lungs and penetrates swiftly
into the brain, producing an almost instantaneous “rush.”
In
the peripheral nervous system, cocaine inhibits voltage-gated sodium channels,
thus blocking initiation and conduction of action potentials . This effect,
however, seems responsible for neither the acute rewarding nor the addictive
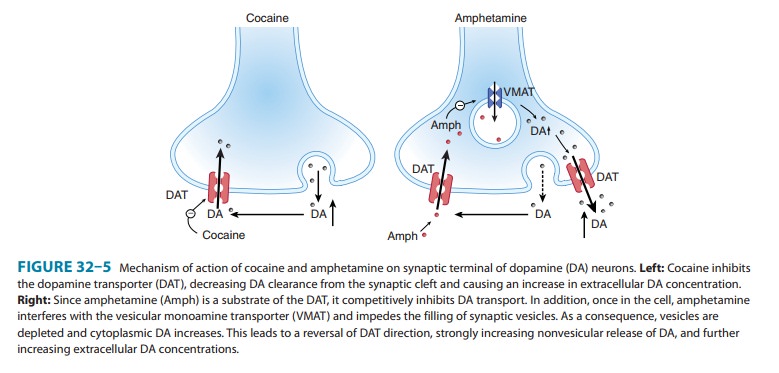
effects. In the central nervous system, cocaine blocks the uptake of dopamine,
noradrenaline, and serotonin through their respective transporters. The block
of the dopamine transporter (DAT),
by increasing dopamine concentrations in the nucleus accumbens, has been
implicated in the rewarding effects of cocaine (Figure 32–5). In fact, the
rewarding effects of cocaine are abolished in mice with a cocaine-insensitive
DAT. The activation of the sympathetic ner-vous system results mainly from
blockage of the norepinephrine transporter (NET) and leads to an acute increase
in arterial pres-sure, tachycardia, and often, ventricular arrhythmias. Users
typi-cally lose their appetite, are hyperactive, and sleep little. Cocaine
exposure increases the risk for intracranial hemorrhage, ischemic stroke,
myocardial infarction, and seizures. Cocaine overdose may lead to hyperthermia,
coma, and death.
Susceptible
individuals may become dependent and addicted after only a few exposures to
cocaine. Although a withdrawal syn-drome is reported, it is not as strong as
that observed with opioids. Tolerance may develop, but in some users a reverse
tolerance is observed; that is, they become sensitized to small doses of
cocaine. This behavioral sensitization is in part context-dependent. Cravings
are very strong and underline the very high addiction liability of cocaine. To
date, no specific antagonist is available, and the management of intoxication
remains supportive. Developing a pharmacologic treatment for cocaine addiction
is a top priority.
AMPHETAMINES
Amphetamines are a group of synthetic, indirect-acting sympath-omimetic drugs that cause the release of endogenous biogenic amines, such as dopamine and noradrenaline. Amphetamine, methamphetamine, and their many derivatives exert their effects by reversing the action of biogenic amine trans-porters at the plasma membrane. Amphetamines are substrates of these transporters and are taken up into the cell (Figure 32–5). Once in the cell, amphetamines interfere with the vesicular mono-amine transporter (VMAT; see Figure 6–4), depleting synaptic vesicles of their neurotransmitter content. As a consequence, levels of dopamine (or other transmitter amine) in the cytoplasm increase and quickly become sufficient to cause release into the synapse by reversal of the plasma membrane DAT.
Normal vesicu-lar release of dopamine consequently
decreases (because synaptic vesicles contain less transmitter), whereas
nonvesicular release increases. Similar mechanisms apply for other biogenic
amines (serotonin and norepinephrine).
Together
with GHB and ecstasy, amphetamines are often referred to as “club drugs,”
because they are increasingly popular in the club scene. They are often
produced in small clandestine laboratories, which makes their precise chemical
identification difficult. They differ from ecstasy chiefly in the context of
use: intravenous administration and “hard core” addiction is far more common
with amphetamines, especially methamphetamine. In general, amphetamines lead to
elevated catecholamine levels that increase arousal and reduce sleep, whereas
the effects on the dop-amine system mediate euphoria but may also cause
abnormal movements and precipitate psychotic episodes. Effects on sero-tonin transmission
may play a role in the hallucinogenic and anorexigenic functions as well as in
the hyperthermia often caused by amphetamines.
Unlike
many other abused drugs, amphetamines are neuro-toxic. The exact mechanism is
not known, but neurotoxicity depends on the NMDA receptor and affects mainly serotonin
and dopamine neurons.
Amphetamines are typically
taken initially in pill form by abusers, but can also be smoked or injected.
Heavy users often progress rap-idly to intravenous administration. Within hours
after oral ingestion, amphetamines increase alertness and cause euphoria,
agitation, and confusion. Bruxism (tooth grinding) and skin flushing may occur.
Effects on heart rate may be minimal with some compounds (eg, methamphetamine),
but with increasing dosage these agents often lead to tachycardia and
dysrhythmias. Hypertensive crisis and vasoconstriction may lead to stroke.
Spread of HIV and hepatitis infection in inner cities has been closely
associated with needle sharing by intravenous users of methamphetamine. With
chronic use, amphetamine tolerance may develop, lead-ing to dose escalation.
Withdrawal consists of dysphoria, drowsi-ness (in some cases, insomnia), and
general irritability.
ECSTASY (MDMA)
Ecstasy is the name of
a class of drugs that includes a large variety of derivatives of the
amphetamine-related compound methylene-dioxymethamphetamine (MDMA). MDMA was
originally used in some forms of psychotherapy, but no medically useful effects
were documented. This is perhaps not surprising, because the main effect of
ecstasy appears to be to foster feelings of intimacy and empathy without
impairing intellectual capacities. Today, MDMA and its many derivatives are
often produced in small quantities in ad hoc laboratories and distributed at
parties or “raves,” where it is taken orally. Ecstasy therefore is the
prototypi-cal designer drug and, as such, is increasingly popular.
Similar to the
amphetamines, MDMA causes release of bio-genic amines by reversing the action
of their respective transport-ers. It has a preferential affinity for the serotonin transporter(SERT) and
therefore most strongly increases the extracellularconcentration of serotonin.
This release is so profound that there is a marked intracellular depletion for
24 hours after a single dose. With repetitive administration, serotonin
depletion may become permanent, which has triggered a debate on its
neurotoxicity. Although direct proof from animal models for neurotoxicity
remains weak, several studies report long-term cognitive impair-ment in heavy
users of MDMA.
In contrast, there is a
wide consensus that MDMA has several acute toxic effects, in particular
hyperthermia, which along with dehydration (eg, caused by an all-night dance
party) may be fatal. Other complications include serotonin syndrome (mental
status change, autonomic hyperactivity, and neuromuscular abnormalities) and
seizures. Following warnings about the dangers of MDMA, some users have
attempted to compensate for hyper-thermia by drinking excessive amounts of
water, causing water intoxication involving severe hyponatremia, seizures, and
even death.
Withdrawal is marked by a
mood “offset” characterized by depression lasting up to several weeks. There
have also been reports of increased aggression during periods of abstinence in
chronic MDMA users.
Taken together, the
evidence for irreversible damage to the brain, although not completely
convincing, implies that even occasional recreational use of MDMA cannot be
considered safe.
Related Topics