Chapter: Essentials of Psychiatry: The Psychiatric Interview: Settings and Techniques
Dimensions of Interviewing Techniques
Dimensions of Interviewing Techniques
Although many systems have been suggested for
classifying in-terview techniques (Elliott et
al., 1987), it is convenient to think about four major dimensions of
interviewing style: degree of di-rectiveness, degree of emotional support,
degree of fact versus feeling orientation and degree of feedback to the
patient. The interviewer must seek a balance among these dimensions to best
cover the needed topics, build rapport, and arrive at a plan of treatment.
Directiveness
Directiveness in the interview ensures that the
necessary areas of information are covered and supplies whatever cognitive
sup-port the patient needs in discussing them. Table 3.6 lists inter-ventions
which are low, moderate and high in directiveness.
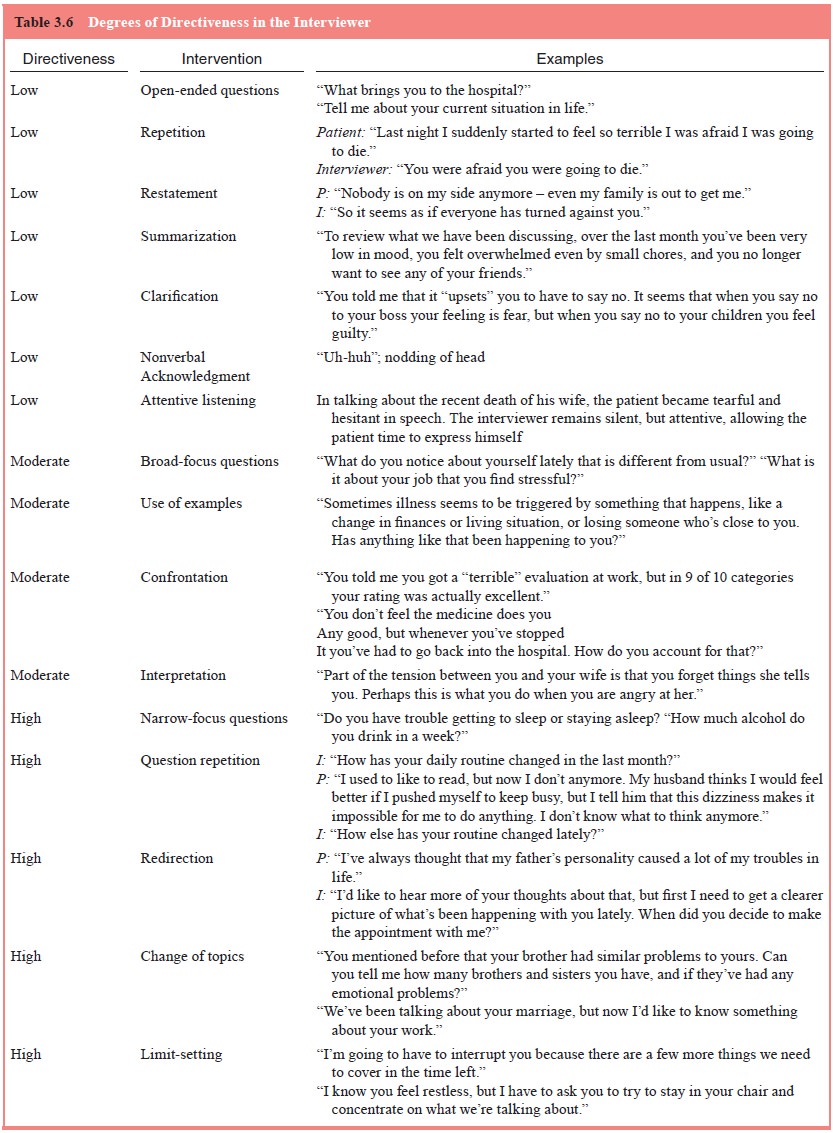
Low-directive interventions request information in
the broadest, most open-ended way and do not go beyond the mate-rial supplied
by the patient. Moderately directive interventions are narrower in focus and
may extend beyond what the patient himself/herself has said. For example, confrontation
makes the patient aware of paradoxes or inconsistencies in the material and
requests him/her to resolve them; interpretation requests the pa-tient to
consider explanations or connections that had not previ-ously occurred to
him/her. Highly directive interventions aim to focus and restrict the patient’s
content or behavior. Such inter-ventions include yes–no or symptom-checklist
type questions and requests for the patient to modify behaviors that impede the
progress of the interview.
Supportiveness
Patients vary considerably in the degree of
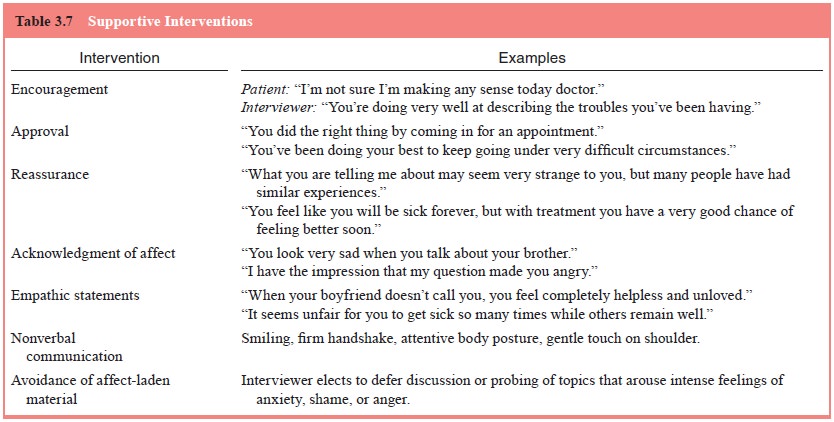
emotional and cogni-tive support they need in the interview. Table 3.7 lists
examples of emotionally supportive interventions. Each such intervention
supports the patient’s sense of security and self-esteem. While some patients
may come to the interview feeling safe and con-fident, others have considerable
anxiety about being criticized, ridiculed, rejected, taken advantage of, or
attacked (literally so in the case of some psychotic patients).
Overt manifestations of insecurity range widely,
from fearful demeanor and tremulousness to requests for reassur-ance to haughty
contemptuousness. The interview’s task is to identify such anxiety when it
arises and respond in a manner.
that conveys empathic understanding, acceptance and
positive regard.
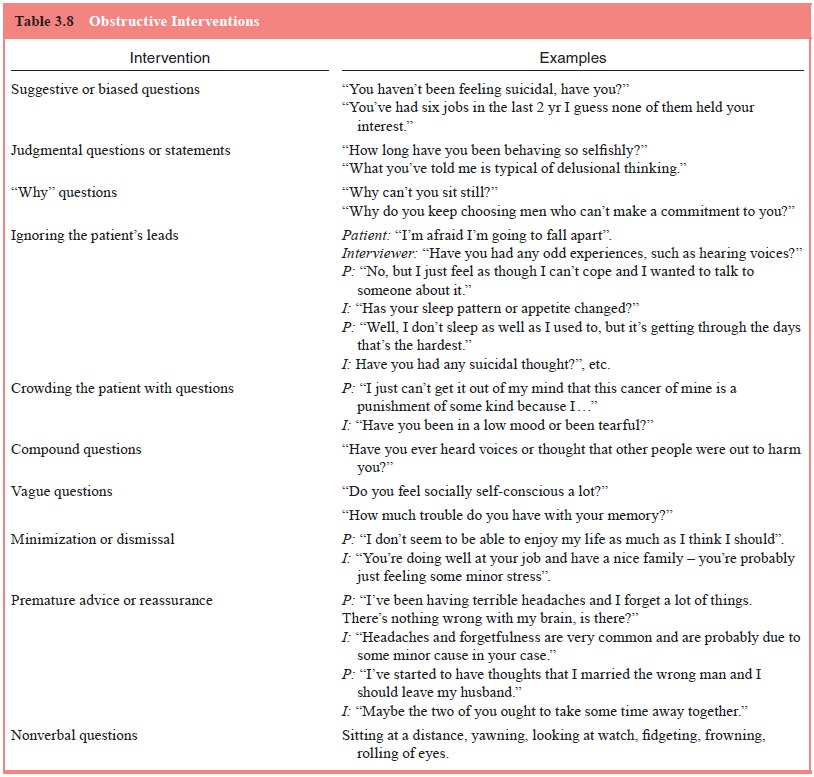
Obstructive interventions are one which (usually
unin-tentionally) impede the flow of information and diminish rap-port. Table
3.8 lists common examples of such interventions. Compound or vague questions
are often confusing to the pa-tient and may produce ambiguous or unclear
answers. Biased or judgmental questions suggest what answer the interviewer
wants to hear or that he/she does not approve of what the pa-tient is saying.
“Why” questions often sound critical or invite rationalizations. “How”
questions better serve the purposes of the interview (“How did you come to
change jobs?” rather than “Why did you change jobs?”). Other interventions are
obstructive because they disregard the patient’s feeling state or what he/she
is trying to say. Paradoxically, this may in-clude premature reassurance or
advice. When given before the interviewer has explored and understood the
issue, this has the effect of cutting off feelings and coming to a premature closure.
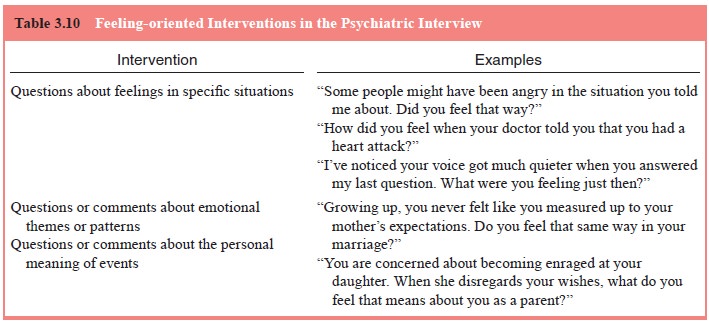
Fact Versus Feeling Orientation
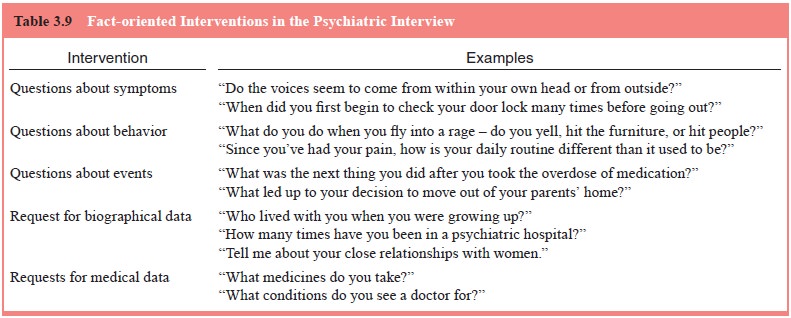
Interviews differ in the degree to which they focus
on factual– objective versus feeling–meaning oriented material. Tables 3.9 and
3.10 provide examples of interventions of both types. The interviewer must
determine what the salient issues are in a given case and develop the focus
accordingly. For example, at one extreme, the principal task in assessing a
cyclically occurring mood disorder might be to delineate precisely the
symptoms, time course and treatment response of the illness. At the other end
of the spectrum might be a patient with a circumscribed dif-ficulty in living,
such as the inability to achieve an intimate, last-ing love relationship. In
such a case, the interviewer may focus not only on the facts of the patient’s
interactions with others but also on the feelings, fantasies and thoughts
associated with such relationships.
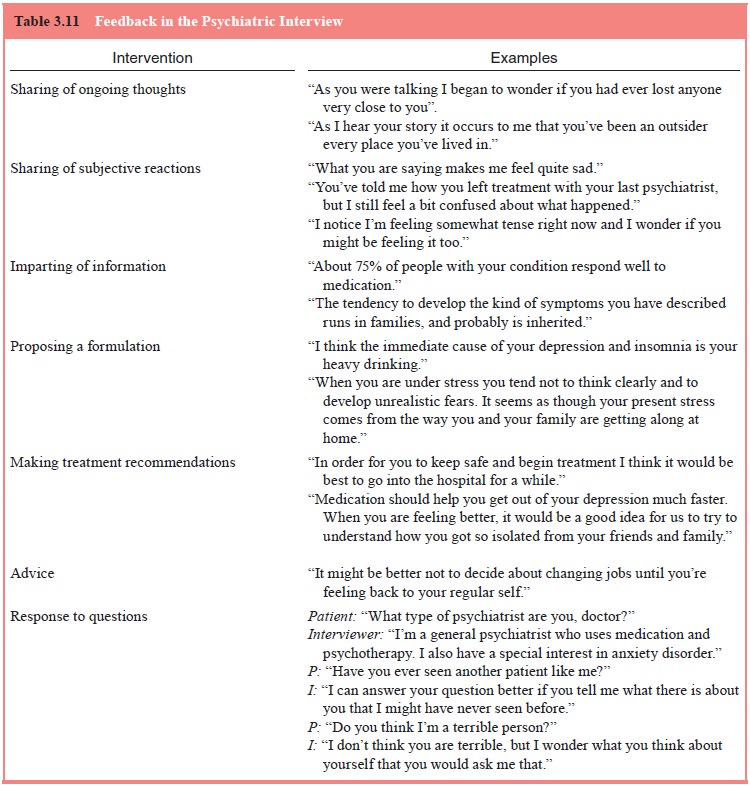
Feedback
Interviews differ in how much the interviewer
conveys to the patient of his/her own thoughts, feelings, conclusions and
rec-ommendations. Table 3.11 presents common types of feedback from the
interviewer. Judicious statements about the interview-er’s ongoing thoughts and
feelings can be used to pose ques-tions or make clarifications or
interpretations while enhanc-ing rapport and trust. Communication of factual
information, formulations of the problem and treatment recommendations are the
foundations of joint treatment planning with the patient. Responding to
questions and giving advice may serve an edu-cational purpose as well as
enhancing the alliance. When re-sponding to requests for advice or information,
the interviewer must first take care to be sure of what is being asked, and for
what reason.
There is little systematic data on the superiority
of one clinical interviewing style over another, but what there are suggest
that many styles can be used effectively. Rutter and his colleagues have
investigated this question in a series of natural-istic and experimental
studies of interviews of parents in a child psychiatry clinic (Rutter et al., 1981; Cox et al., 1981, 1988). The major findings of these studies are:
· Active,
structured techniques are no better than nondirec-tive styles in eliciting
positive findings (i.e., areas of pathol-ogy). However, active techniques are
better in eliciting more detailed and thorough information in areas where
pathol-ogy is found and are also better at delineating areas without pathology.
· An
active, fact-gathering style does not prevent the inter-viewer from effectively
eliciting emotional reactions from informants.
· Use of open questions, direct requests for feelings, interpreta-tions of feelings, and expressions of sympathy are associated with greater expression of emotions by informants.
· Less
activity on the interviewer’s part is associated with more informant
talkativeness and spontaneous emotional expres-sion. Less directive techniques
also tend to produce more emotional responses at times when they are not
specifically requested. Conversely, more active styles of asking about feelings
may be more effective for informants who are low in spontaneous emotional expression.
·
In summary, techniques which actively elicit both
facts and emotions are likely to produce the richest, most detailed da-tabase.
When skillfully used, these do not impair the doctor– patient relationship.
Related Topics