Chapter: Essentials of Anatomy and Physiology: The Senses
Cutaneous Senses
CUTANEOUS SENSES
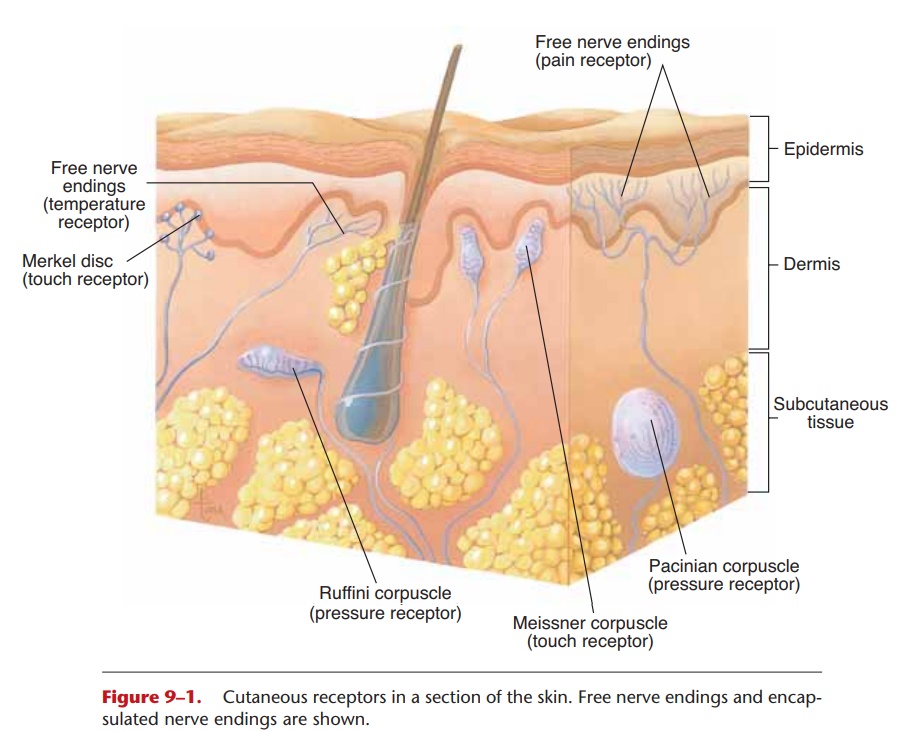
The dermis of the skin and the subcutaneous tissue contain receptors for the sensations of touch, pressure, heat, cold, and pain. The receptors for pain, heat, and cold are free nerve endings, which also respond to any intense stimulus. Intense pressure, for example, may be felt as pain. The receptors for touch and pres-sure are encapsulated nerve endings, meaning that there is a cellular structure around the nerve ending (Fig. 9–1).
The cutaneous senses provide us with informa-tion about the external environment and also about the skin itself. Much of the information about the environment is not of great importance and is processed at a subconscious level (suppressed by the thalamus), though we can choose to be aware of it. For example, could you distinguish a cotton T-shirt from denim jeans by touch alone? Probably, but you might not realize that you can do that until you try it by, say, sorting laundry in the dark.
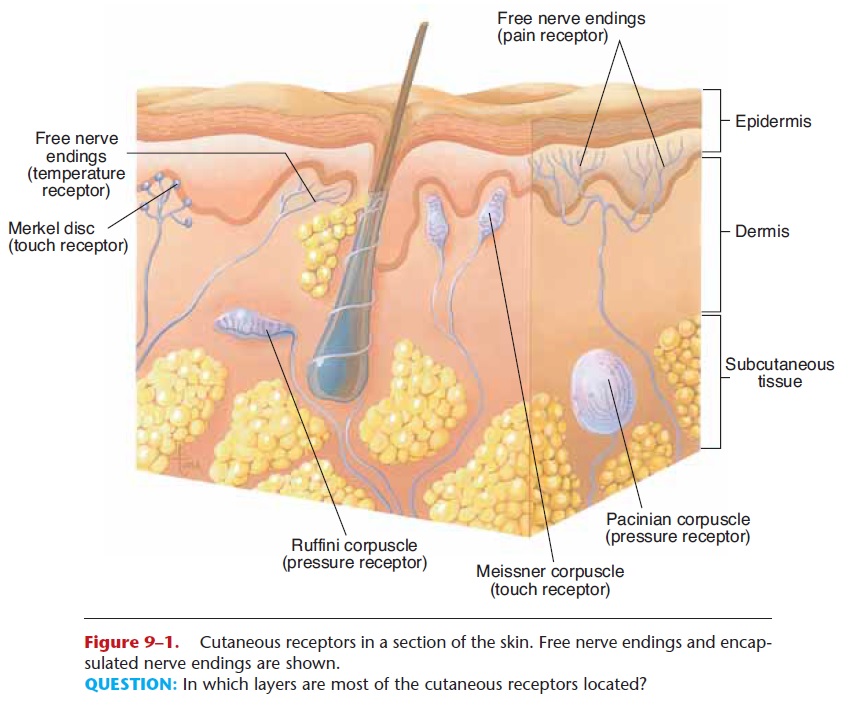
Figure 9–1. Cutaneous receptors in a section of the skin. Free nerve endings and encap-sulated nerve endings are shown.
QUESTION: In which layers are most of the cutaneous receptors located?
If you were walking bare-foot, could you tell if you were walking on a carpet, a wood floor, concrete, or beach sand? Yes, you could. But are we usually aware of the sensation from the soles of our feet? If all is going well, probably not. Some people with diabetes develop diabetic neuropa-thy, damage to nerves that impairs sensation, and theymay say that a wood floor feels like walking on cotton balls or that the buttons of a shirt feel too large or too small. They are aware of such odd sensations simply because the feelings are odd. For most of us, the touch of the wood floor is not brought to awareness because it is what the brain expects from past experience, but if the floor has splinters or if the beach sand is hot, we are certainly aware. This is information we can bring to our conscious minds if necessary, but usually do not.
As for the skin itself, if you have ever had poison ivy or chickenpox, you may remember the itching sensa-tion of the rash. An itch is actually a mild pain sensa-tion, which may become real pain if not scratched. Why does scratching help relieve some itches, besides by removing an external irritant? One proposed mechanism is that scratching is a bit more painful than the itch, and the impulses it generates can distract the brain from the impulses from the itch. Scratching will not help relieve the itch of poison ivy, chickenpox, or a mosquito bite, however, because the irritating chem-icals are in the skin, not on it. In such cases, scratch-ing may do more damage and worsen inflammation at the site.
The sensory areas for the skin are in the parietal lobes. You may recall that the sensi-tivity of an area of skin is determined by the number of receptors present. The number of receptors corre-sponds to the size of the sensory area in the cerebral cortex. The largest parts of this sensory cortex are for the parts of the skin with the most receptors, that is, the hands and face.
As mentioned previously, sensory areas are not merely passive recipients of impulses. Consider the sensation of wetness. It is a distinct sensation, but there are no receptors for “wet” in the skin. Where does the sensation come from? Where all sensation comes from: the brain. The parietal lobes have learned to associate the simultaneous reception of temperature and pressure impulses with “wet.” You can demon-strate this for yourself by putting on a plastic glove and dunking your fingers in a cup of water. Your fin-gers will feel wet, though they are perfectly dry inside the glove. Wetness is a learned sensation, created by the brain.
REFERRED PAIN
Free nerve endings are also found in internal organs. The smooth muscle of the small intestine, for exam-ple, has free nerve endings that are stimulated by excessive stretching or contraction; the resulting pain is called visceral pain. Sometimes pain that originates in an internal organ may be felt in a cutaneous area; this is called referred pain. The pain of a heart attack (myocardial infarction) may be felt in the left arm and shoulder, or the pain of gallstones may be felt in the right shoulder.
This referred pain is actually a creation of the brain. Within the spinal cord are sensory tracts that are shared by cutaneous impulses and visceral impulses. Cutaneous impulses are much more fre-quent, and the brain correctly projects the sensation to the skin. When the impulses come from an organ such as the heart, however, the brain may still project the sensation to the “usual” cutaneous area. The brain projects sensation based on past experience, and cuta-neous pain is far more common than visceral pain. Knowledge of referred pain, as in the examples men-tioned earlier, may often be helpful in diagnosis.
Related Topics