Chapter: Case Study in Obstetrics and Gynaecology: Emergency Gynaecology
Case Study Reports: Abdominal Pain
ABDOMINAL PAIN
History
A
24-year-old student is referred to the gynaecologist on call from the emergency depart- ment with sudden-onset of left iliac
fossa pain which
woke her at 2 am.
She fell asleep again but since 8 am the
pain has been
constant and is not relieved by ibuprofen or cody-
dramol.
Her
last period started
2 weeks ago and she reports no irregular bleeding
or discharge. She has no significant gynaecological history except
for a termination of pregnancy age 17 years. She has been with her current boyfriend for 2 years
and has used the combined oral contraceptive pill (COCP)
throughout that time.
She says she
has not had
intercourse for the last
4 months because
her boyfriend has
been travelling, but
says that intercourse has never been painful.
On
direct questioning she has felt nauseated but has not vomited. She has had no urinary symptoms but has opened
her bowels several
times each day
for the last
3 days, which
is unusual for her.
Examination
On
examination she is apyrexial, her observations are normal and her abdomen
is soft with vague
left iliac fossa
tenderness but no signs of peritonism. Bimanual examination reveals a normal-sized uterus with no adnexal tenderness or cervical excitation and no obvious
adnexal masses.
Questions
·
What is the first investigation you would like to perform?
·
What is your differential diagnosis if this test is negative, and how would
you rule out some of these diagnoses?
ANSWER
Any
woman of reproductive age with abdominal pain should always
have a urinary
preg- nancy test, regardless of the date
of her last
menstrual period. In this case
the test is negative.
The remaining differential diagnoses
include:
·
ovarian cyst
·
pelvic inflammatory disease
·
urinary tract infection or stone
·
bowel-related cause.
There are no specific
gynaecological symptoms or adnexal tenderness, which implies that the
pain is not
gynaecological in origin.
However, during speculum examination it is pru-
dent to send swabs for chlamydial and gonorrhoeal infection opportunistically, in view of
the high background prevalence of sexually transmitted infection, especially in the
18–25-year-old age group.
Ovulation pain (mittelschmirtz) or a corpus
luteal cyst are
very unlikely as the COCP inhibits the ovulatory cycle.
However, a transvaginal ultrasound scan will rule out an ovarian cyst for certain.
Urine should be dipped
for blood to rule out
a renal stone,
and for leucocytes and nitrites to
rule out infection.
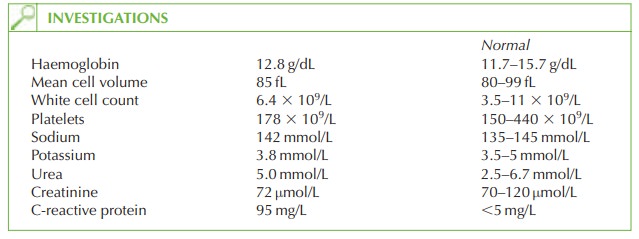
Bowel habit is altered
and the raised
C-reactive protein suggests an inflammatory condi- tion. As the onset
is acute and not severe,
the diagnosis is likely to be gastroenteritis. This should be managed
expectantly, with fluids,
rest and simple analgesia. A stool culture should be sent if the symptoms fail to resolve. Other inflammatory bowel
conditions such as Crohn’s
disease and ulcerative colitis are rare
causes to consider if the symptoms are persistent or recurrent.
Irritable bowel syndrome is not associated with raised inflammatory markers, and is there-
fore not a differential diagnosis in this case.

Related Topics