Chapter: Case Study in Obstetrics and Gynaecology: Emergency Gynaecology
Case Study Reports: Abdominal Pain
ABDOMINAL PAIN
History
A
26-year-old woman presents with abdominal pain.
It started suddenly 2 h ago
and was initially in the lower
abdomen but is now generalized. She feels nauseated and dizzy,
especially when she sits up. She also feels as if she has bruised
her shoulder. She has not noticed any vaginal bleeding or discharge, and
there are no bowel or urinary symptoms.
She
does not keep a record
of her period dates but thinks the last one was about
a month ago. She has a regular partner
and says that they often
forget to use a condom.
She had a termination 3 years ago.
She was diagnosed with chlamydia when she was admitted to hospital at the age
of 19 years with a pelvic infection.
There is no other medical history of
note.
Examination
On
examination she is pale and looks unwell.
She is intermittently drowsy. She is lying flat and still on the bed. The temperature is 35.9°C, pulse
120/min and blood
pressure 95/50 mmHg. Peripherally she is cool
and the hands
are clammy. She
is generally slim
but the abdomen is symmetrically distended. There is generalized tenderness on light
palpa- tion, with rebound
tenderness and guarding. There are no obviously palpable
masses and vaginal examination has not been carried out.
Urinary pregnancy test: positive
Questions
·
What is the likely diagnosis?
·
How would you manage the patient?
Answer:
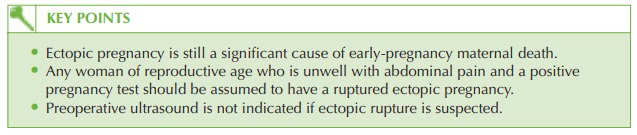
Any
woman who is unwell with abdominal pain should be assumed to have a ruptured
ectopic pregnancy. In this case
there are risk
factors and the
symptoms of dizziness, nau- sea, severe abdominal pain and shoulder pain are
classical of haemoperitoneum. The
examination findings of cool and clammy peripheries, a distended abdomen,
tachycardia and hypotension also suggest the clinical diagnosis
and a positive pregnancy test confirms
this.
Young women tend
to compensate for
hypovolaemia, and the
fact that this
woman is now cool and clammy with hypotension suggests
that she is gravely unwell
and should be transferred for definitive management without delay.
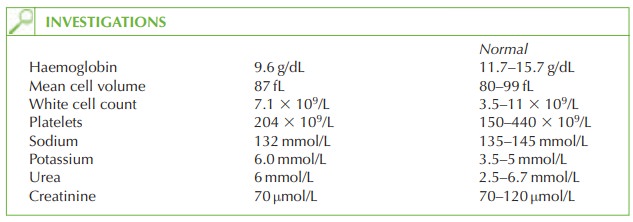
Although the haemoglobin does
not seem dramatically reduced, it is likely that
on repeat testing it may now
be extremely low.
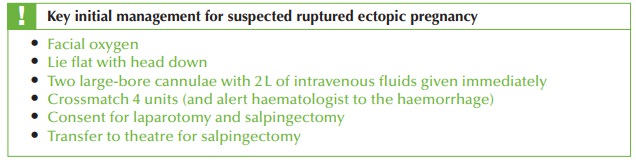
Management
The
anaesthetist, theatre staff
and senior gynaecologist should be alerted
immediately and the woman
transferred to theatre
for surgery. An ultrasound is not necessary and would increase the
threat to this
woman by increasing the delay in reaching theatre.
Ruptured ectopic pregnancy is still
the leading cause of maternal death in early
preg- nancy, and doctors must be alert to the occasional presentation
with life-threatening haemorrhage, as in this
case.
Related Topics