Chapter: Medical Surgical Nursing: Management of Patients With Chronic Obstructive Pulmonary Disease
Bronchiectasis
Bronchiectasis
Bronchiectasis is
a chronic, irreversible dilation of the bronchiand bronchioles. Under the new
definition of COPD, it is considered a separate disease process from COPD (NIH,
2001). Bronchiectasis may be caused by a variety of conditions, including:
·
Airway obstruction
·
Diffuse airway injury
·
Pulmonary infections and obstruction
of the bronchus or complications of long-term pulmonary infections
·
Genetic disorders such as cystic
fibrosis
·
Abnormal host defense (eg, ciliary
dyskinesia or humoral immunodeficiency)
·
Idiopathic causes
A
person may be predisposed to bronchiectasis as a result of recurrent respiratory
infections in early childhood, measles, in-fluenza, tuberculosis, and
immunodeficiency disorders.
Pathophysiology
The
inflammatory process associated with pulmonary infections damages the bronchial
wall, causing a loss of its supporting struc-ture and resulting in thick sputum
that ultimately obstructs the bronchi. The walls become permanently distended
and distorted, impairing mucociliary clearance. The inflammation and infection
extend to the peribronchial tissues; in the case of saccular bronchiectasis,
each dilated tube virtually amounts to a lung ab-scess, the exudate of which
drains freely through the bronchus. Bronchiectasis is usually localized,
affecting a segment or lobe of a lung, most frequently the lower lobes.
The
retention of secretions and subsequent obstruction ulti-mately cause the
alveoli distal to the obstruction to collapse (at-electasis). Inflammatory
scarring or fibrosis replaces functioning lung tissue. In time the patient
develops respiratory insufficiency with reduced vital capacity, decreased
ventilation, and an increased ratio of residual volume to total lung capacity.
There is impair ment in the matching of ventilation to perfusion (ventilation–
perfusion imbalance) and hypoxemia.
Clinical Manifestations
Characteristic
symptoms of bronchiectasis include chronic cough and the production of purulent
sputum in copious amounts. Many patients with this disease have hemoptysis.
Clubbing of the fingers also is common because of respiratory insufficiency.
The patient usually has repeated episodes of pulmonary infection. Even with
modern treatment approaches, the average age at death is approximately 55
years.
Assessment and Diagnostic Findings
Bronchiectasis
is not readily diagnosed because the symptoms can be mistaken for those of
simple chronic bronchitis. A definite sign is offered by the prolonged history
of productive cough, with sputum consistently negative for tubercle bacilli.
The diagnosis is established by a computed tomography (CT) scan, which
demon-strates either the presence or absence of bronchial dilation.
Medical Management
Treatment
objectives are to promote bronchial drainage to clear excessive secretions from
the affected portion of the lungs and to prevent or control infection. Postural
drainage is part of all treat-ment plans because draining the bronchiectatic
areas by gravity reduces the amount of secretions and the degree of infection.
Sometimes mucopurulent sputum must be removed by bron-choscopy. Chest
physiotherapy, including percussion and pos-tural drainage, is important in
secretion management.
Smoking
cessation is important because smoking impairs bronchial drainage by paralyzing
ciliary action, increasing bron-chial secretions, and causing inflammation of
the mucous mem-branes, resulting in hyperplasia of the mucous glands. Infection
is controlled with antimicrobial therapy based on the results of sen-sitivity
studies on organisms cultured from sputum. A year-round regimen of antibiotic
agents may be prescribed, with different types of antibiotics at intervals.
Some clinicians prescribe anti-biotic agents throughout the winter or when
acute upper respira-tory tract infections occur. Patients should be vaccinated
against influenza and pneumococcal pneumonia. Bronchodilators, which may be
prescribed for patients who also have reactive airway dis-ease, may also assist
with secretion management.
Surgical
intervention, although used infrequently, may be in-dicated for the patient who
continues to expectorate large amounts of sputum and has repeated bouts of
pneumonia and he-moptysis despite adhering to the treatment regimen. However,
the disease must involve only one or two areas of the lung that can be removed
without producing respiratory insufficiency. The goals of surgical treatment
are to conserve normal pulmonary tis-sue and to avoid infectious complications.
Diseased tissue is re-moved, provided that the postoperative lung function will
be adequate. It may be necessary to remove a segment of a lobe (segmental
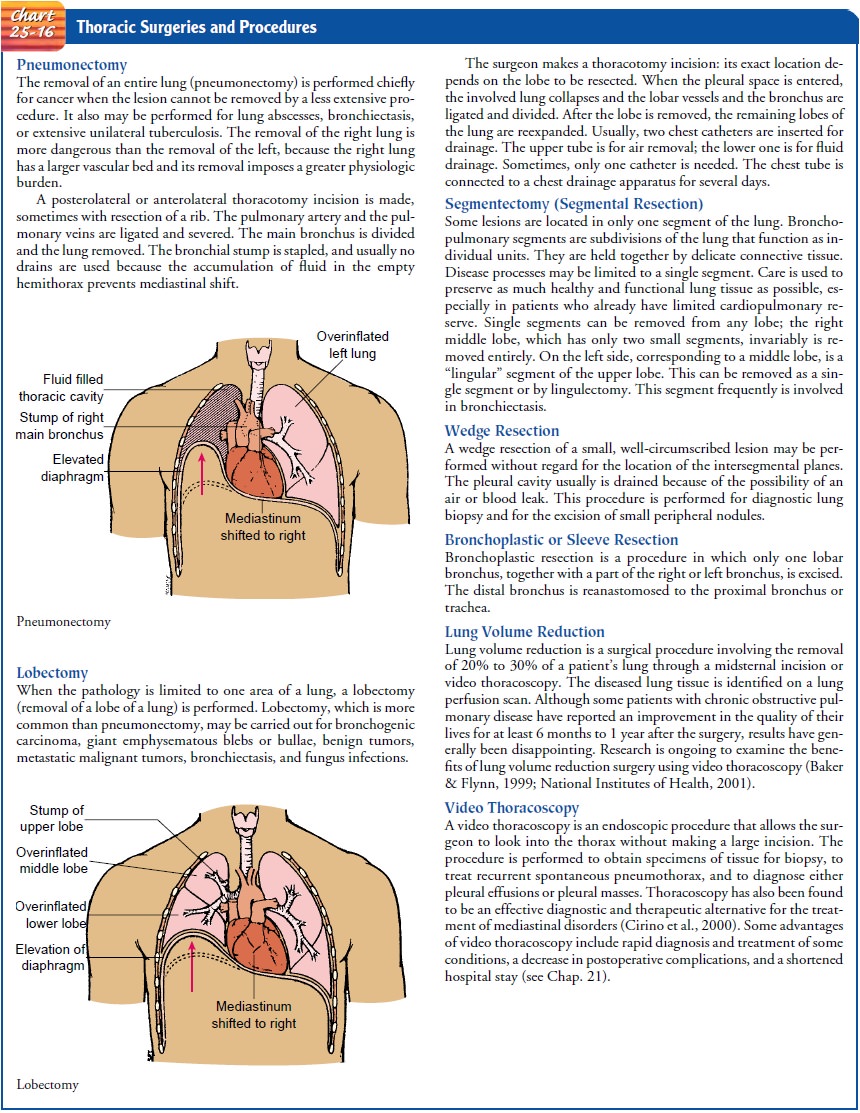
resection), a lobe (lobectomy), or rarely an entire lung (pneumonectomy). (See
Chart 25-16 for further information.) Segmental resection is the removal of an
anatomic subdivision of a pulmonary lobe. The chief advantage is that only
diseased tis-sue is removed and healthy lung tissue is conserved.
The
surgery is preceded by a period of careful preparation. The objective is to
obtain a dry (free of infection) tracheo-bronchial tree to prevent
complications (atelectasis, pneumonia, bronchopleural fistula, and empyema).
This is accomplished by postural drainage or, depending on the location, by
direct suction through a bronchoscope. A course of antibacterial therapy may be
prescribed. After surgery, the care is the same as for any patient undergoing
chest surgery.
Nursing Management
Nursing
management of the patient with bronchiectasis focuses on alleviating symptoms
and assisting the patient to clear pul-monary secretions. Smoking and other
factors that increase the production of mucus and hamper its removal are
targeted in pa-tient teaching. The patient and family are taught to perform
pos-tural drainage and to avoid exposure to others with upper respiratory and
other infections. If the patient experiences fa-tigue and dyspnea, strategies
to conserve energy while maintain-ing as active a lifestyle as possible are
discussed. The patient needs to become knowledgeable about early signs of
respiratory infection and the progression of the disorder so that appropriate
treatment can be implemented promptly. Because the presence of a large amount
of mucus may decrease the patient’s appetite and result in an inadequate
dietary intake, the patient’s nutritional status is assessed and strategies are
implemented to ensure an ad-equate diet.
Related Topics