Chapter: Essentials of Anatomy and Physiology: Skeletal System: Bones and Joints
Axial Skeleton
AXIAL SKELETON
Skull
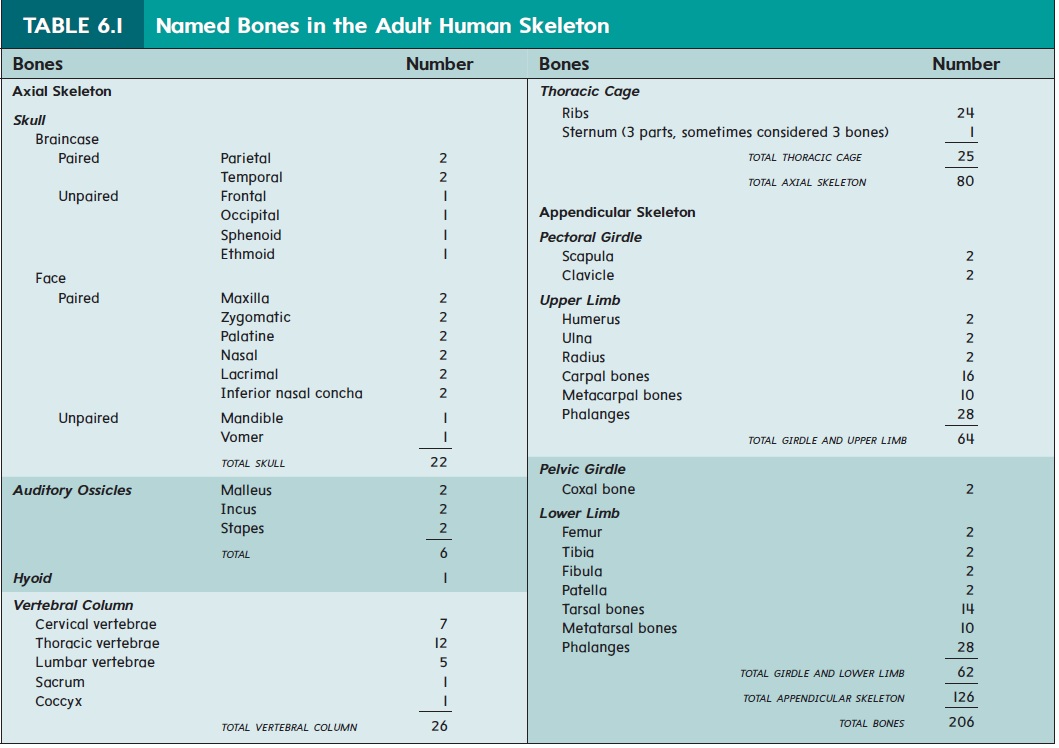
The 22 bones of the skull are divided into those of the braincase and those of the face (see table 6.1). The braincase, which enclos-es the cranial cavity, consists of 8 bones that immediately surround and protect the brain; 14 facial bones form the structure of the face. Thirteen of the facial bones are rather solidly connected to form the bulk of the face. The mandible, however, forms a freely movable joint with the rest of the skull. There are also three audi-tory ossicles (os′\i-klz) in each middle ear (six total).
Many students studying anatomy never see the individual bones of the skull. Even if they do, it makes more sense from a functional, or clinical, perspective to study most of the bones as they appear together in the intact skull because many of the anatomical features of the skull cannot be fully appreciated by examining the separate bones. For example, several ridges on the skull cross more than one bone, and several foramina are located between bones rather than within a single bone. For these reasons, it is more relevant to think of the skull, excluding the mandible, as a single unit. The major features of the intact skull are therefore described from four views.
Lateral View
The parietal bones (pă-rı̄ ′\ĕ-tăl; wall) and temporal (tem′\pō-răl) bones form a large portion of the side of the head (figure 6.11). (Theword temporal refers to time, and the temporal bone is so named because the hairs of the temples turn white, indicating the passage of time.) These two bones join each other on the side of the head at the squamous (skwā′\mŭs) suture. A suture is a joint uniting bones of the skull. Anteriorly, the parietal bone is joined to the frontal (forehead) bone by the coronal (kōr′\ō-năl; corona, crown) suture, and posteriorly it is joined to the occipital (ok-sip′\i-tăl; back of the head) bone by the lambdoid (lam′\doyd) suture. A prominent feature of the temporal bone is a large opening, the external auditory canal, a canal that enables sound waves to reach the eardrum. The mastoid (mas′\toyd)process of the temporal bone can be seen and felt as a prominent lump just posterior to the ear. Important neck muscles involved in rotation of the head attach to the mastoid process.
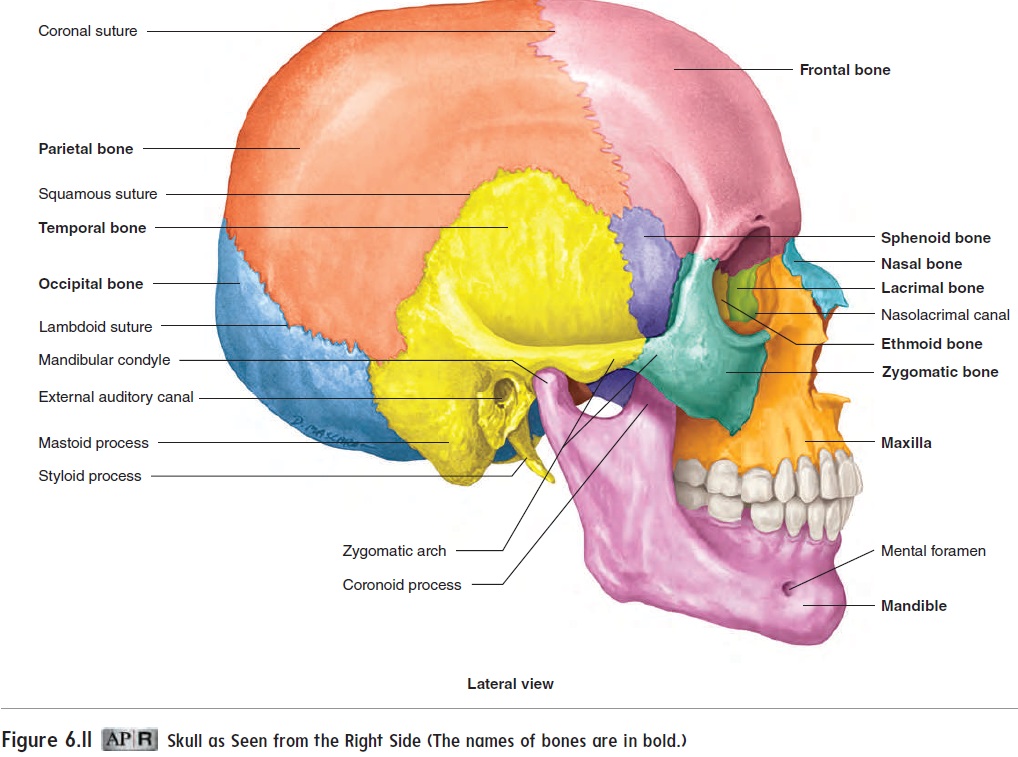
Part of the sphenoid (sfē′\noyd) bone can be seen immedi-ately anterior to the temporal bone. Although it appears to be two small, paired bones on the sides of the skull, the sphenoid bone is actually a single bone that extends completely across the skull. It resembles a butterfly, with its body in the center of the skull and its wings extending to the sides of the skull. Anterior to the sphenoid bone is the zygomatic(zı̄-gō-mat′\ik) bone, or cheekbone, which can be easily felt. The zygomatic arch, which consists of joined processes of the temporal and zygomatic bones, forms a bridge across the side of the face and provides a major attachment site for a muscle moving the mandible.
The maxilla (mak-sil′\ă; jawbone) forms the upper jaw, and the mandible (man′\di-bl; jaw) forms the lower jaw. The maxilla articu-lates by sutures to the temporal bone. The maxilla contains the supe-rior set of teeth, and the mandible contains the inferior set of teeth.
Frontal View
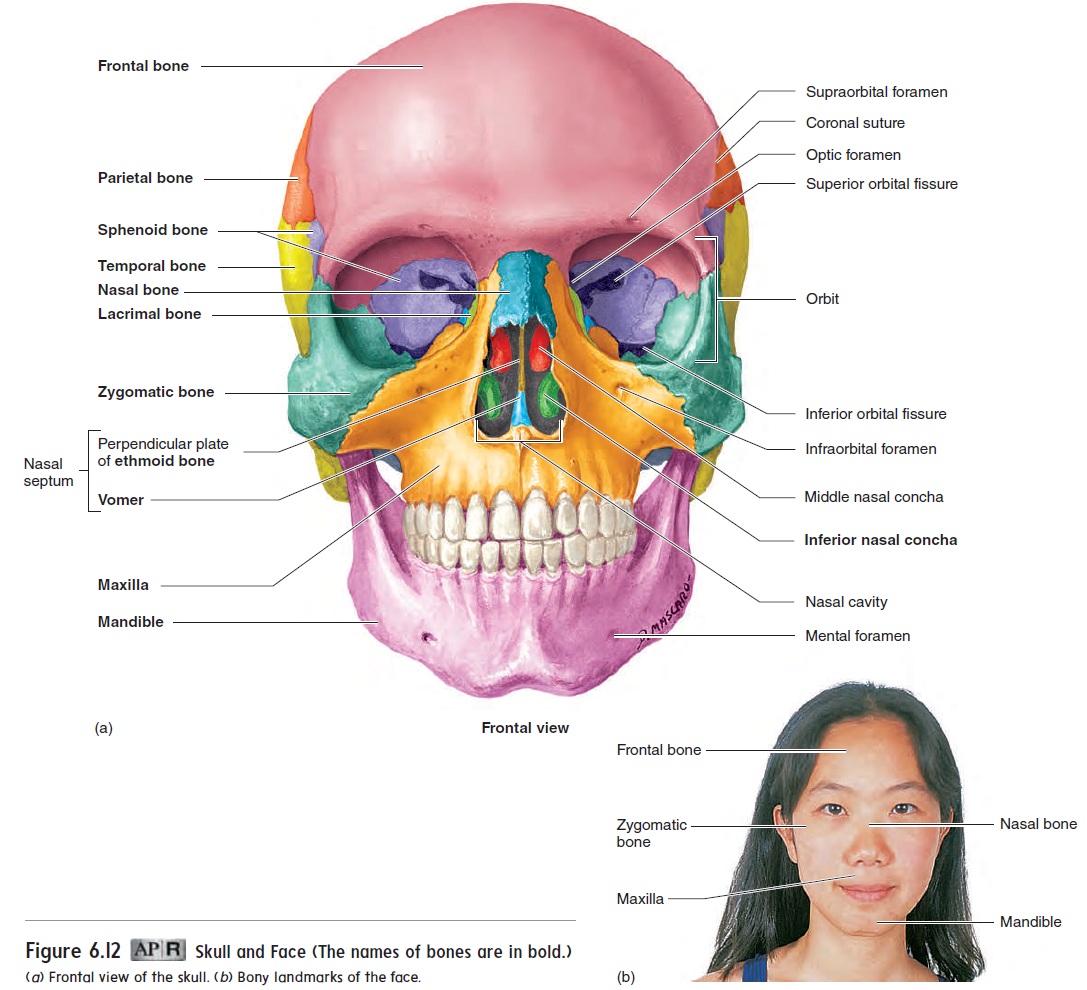
The major structures seen from the frontal view are the frontal bone, the zygomatic bones, the maxillae, and the mandible (figure 6.12a). The teeth are very prominent in this view. Many bones of the face can be easily felt through the skin (figure 6.12b).
Skull as Seen from the Right Side (The names of bones are in bold.)
From this view, the most prominent openings into the skull are the orbits (̄o r′ bitz; eye sockets) and the nasal cavity. The orbits are cone-shaped fossae, so named because the eyes rotate within them. The bones of the orbits provide both protection for the eyes and attachment points for the muscles that move the eyes. The orbit is a good example of why it is valuable to study the skull as an intact structure. No fewer than seven bones come together to form the orbit, and for the most part, the contribution of each bone to the orbit cannot be appreciated when the bones are examined individually.
Each orbit has several openings through which structures communicate with other cavities (figure 6.12a). The largest of these are the superior and inferior orbital fissures. They provide openings through which nerves and blood vessels communicate with the orbit or pass to the face. The optic nerve, for the sense of vision, passes from the eye through the optic foramen and enters the cranial cavity. Thenasolacrimal (nā -zō -lak′ ri-mă l; nasus, nose + lacrima, tear) canal (see figure 6.11) passes from the orbit into the nasal cavity. It contains a duct that carries tears from the eyes to the nasal cavity. A smalllacrimal (lak′ ri-mă l) bone can be seen in the orbit just above the opening of this canal.
The nasal cavity is divided into right and left halves by a nasal septum (sep′tŭm; wall) (figure 6.12a). The bony part of thenasal septum consists primarily of the vomer (vō ′ mer) inferiorly and theperpendicular plate of the ethmoid (eth′ moyd; sieve-shaped) bone superiorly. The anterior part of the nasal septum is formed by cartilage.
The external part of the nose is formed mostly of cartilage. The bridge of the nose is formed by the nasal bones.
Each of the lateral walls of the nasal cavity has three bony shelves, called the nasal conchae (kon′ k̄e ; resembling a conch shell). The inferior nasal concha is a separate bone, and the middle and superior conchae are projections from the ethmoid bone. The conchae increase the surface area in the nasal cavity. The increased surface area of the overlying epithelium facilitates moistening and warming of the air inhaled through the nose .
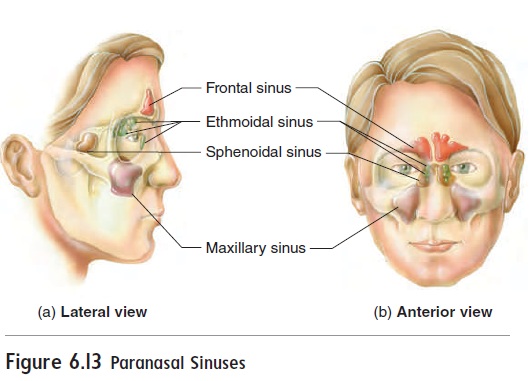
Several of the bones associated with the nasal cavity have large cavities within them, called the paranasal (par-̆a -n̄a ′ s̆a l; para, alongside) sinuses (figure 6.13), which open into the nasal cavity. The sinuses decrease the weight of the skull and act as resonating chambers during voice production. Compare a normal voice with the voice of a person who has a cold and whose sinuses are “stopped up.” The sinuses are named for the bones where they are located and include the frontal, maxillary, ethmoidal, and sphenoidal sinuses
The skull has additional sinuses, called the mastoid air cells, which are located inside the mastoid processes of the temporal bone. These air cells open into the middle ear instead of into the nasal cavity. An auditory tube connects the middle ear to the naso-pharynx (upper part of throat).
Interior of the Cranial Cavity
When the floor of the cranial cavity is viewed from above with the roof cut away (figure 6.14), it can be divided roughly into three cranial fossae (anterior, middle, and posterior), which are formed as the developing skull conforms to the shape of the brain. The bones forming the floor of the cranial cavity, from anterior to pos-terior, are the frontal, ethmoid, sphenoid, temporal, and occipital bones. Several foramina can be seen in the floor of the middle fossa. These allow nerves and blood vessels to pass through the skull. For example, the foramen rotundum and foramen ovale transmit important nerves to the face. A major artery to the menin-ges (the membranes around the brain) passes through the foramen spinosum. The internal carotid artery passes through the carotid canal, and the internal jugular vein passes through the jugular foramen . The large foramen magnum, through which the spinal cord joins the brain, is located in the posterior
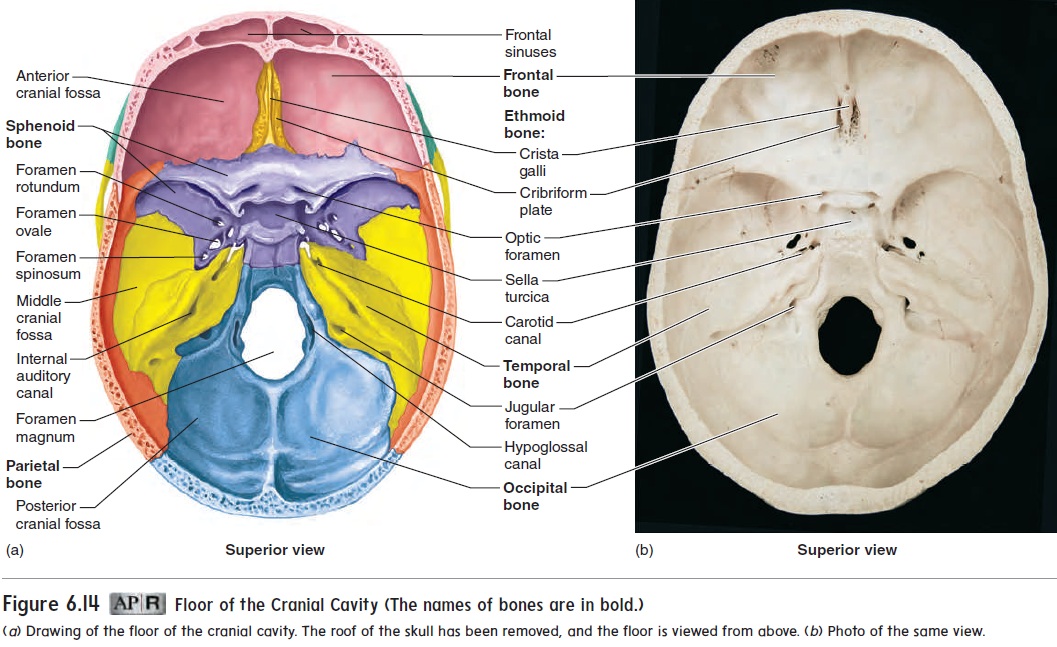
fossa. The central region of the sphenoid bone is modified into a structure resembling a saddle, the sella turcica (sel′ ̆a t̆u r′ s -k̆a ; Turkish saddle), which contains the pituitary gland.
Base of Skull Viewed from Below
Many of the same foramina that are visible in the interior of the skull can also be seen in the base of the skull, when viewed from below, with the mandible removed (figure 6.15). Other specialized structures, such as processes for muscle attachments, can also be seen. The foramen magnum is located in the occipital bone near the center of the skull base. Occipital condyles (ok-sip′ i-t̆a l kon′ dı̄ lz), the smooth points of articulation between the skull and the vertebral column, are located beside the foramen magnum.
Two long, pointed styloid (stı̄ ′ loyd; stylus or pen-shaped) processes project from the inferior surface of the temporal bone.The muscles involved in moving the tongue, the hyoid bone, and the pharynx (throat) originate from this process. The mandibularfossa, where the mandible articulates with the temporal bone, isanterior to the mastoid process.
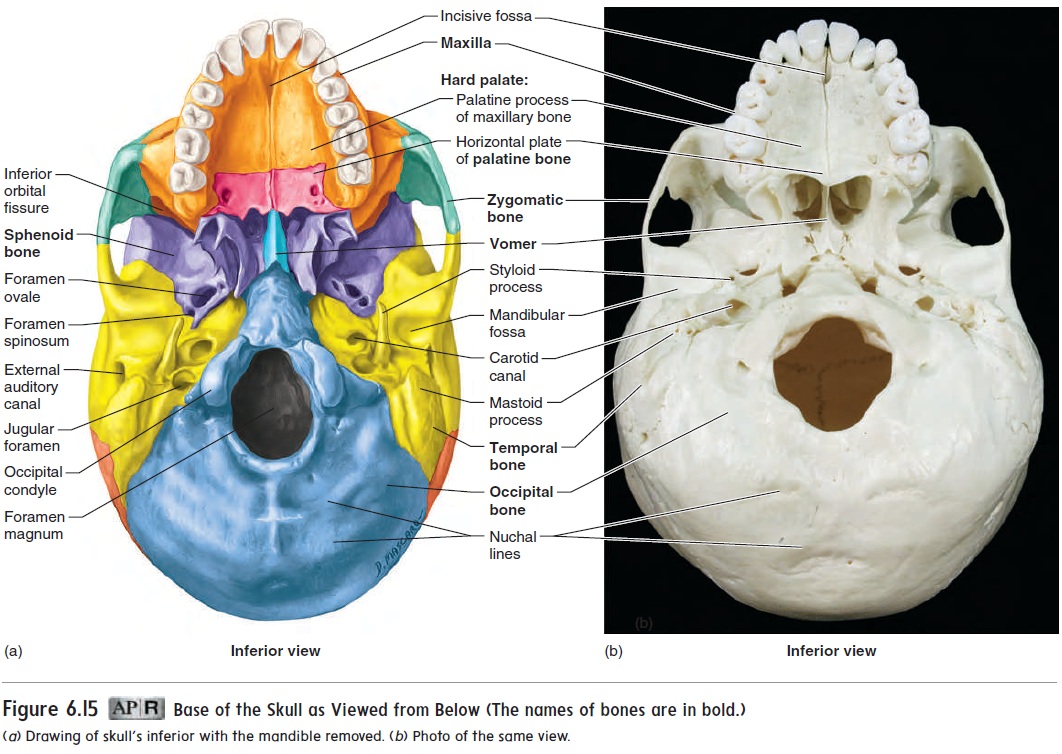
The hard palate (pal′ ă t) forms the floor of the nasal cavity and the roof of the mouth. The anterior two-thirds of the hard palate is formed by the maxillae, the posterior one-third by the palatine (pal′ă-tı̄n)bones. The connective tissue and muscles thatmake up the soft palate extend posteriorly from the hard, or bony, palate. The hard and soft palates separate the nasal cavity and nasopharynx from the mouth, enabling us to chew and breathe at the same time.
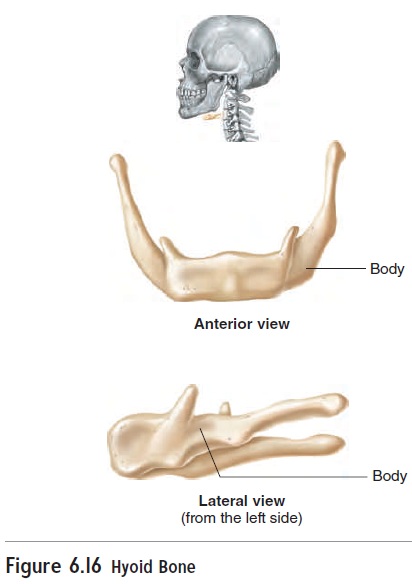
Hyoid Bone
The hyoid bone (figure 6.16) is an unpaired, U-shaped bone. It is not part of the skull (see table 6.1) and has no direct bony attach-ment to the skull. Muscles and ligaments attach it to the skull. The hyoid bone provides an attachment for some tongue muscles, and it is an attachment point for important neck muscles that elevate the larynx (voicebox) during speech or swallowing.
Vertebral Column
The vertebral column, or backbone, is the central axis of the skeleton, extending from the base of the skull to slightly past the end of the pelvis. In adults, it usually consists of 26 individ-ual bones, grouped into five regions (figure 6.17; see table 6.1): 7 cervical (ser′ vı̆ -kal; neck) vertebrae (ver′ t ĕ -brē ; verto, to turn), 12 thoracic (th̄o -ras′ ik) vertebrae, 5 lumbar (l̆u m′ bar) vertebrae,1 sacral (sā ′ kră l)bone, and 1 coccyx (kok′ siks) bone. The adult sacral and coccyx bones fuse from 5 and 3–4 individual bones, respectively. For convenience, each of the five regions is identified by a letter, and the vertebrae within each region are numbered: C1–C7, T1–T12, L1–L5, S, and CO. You can remember the num-ber of vertebrae in each region by remembering meal times: 7, 12, and 5.
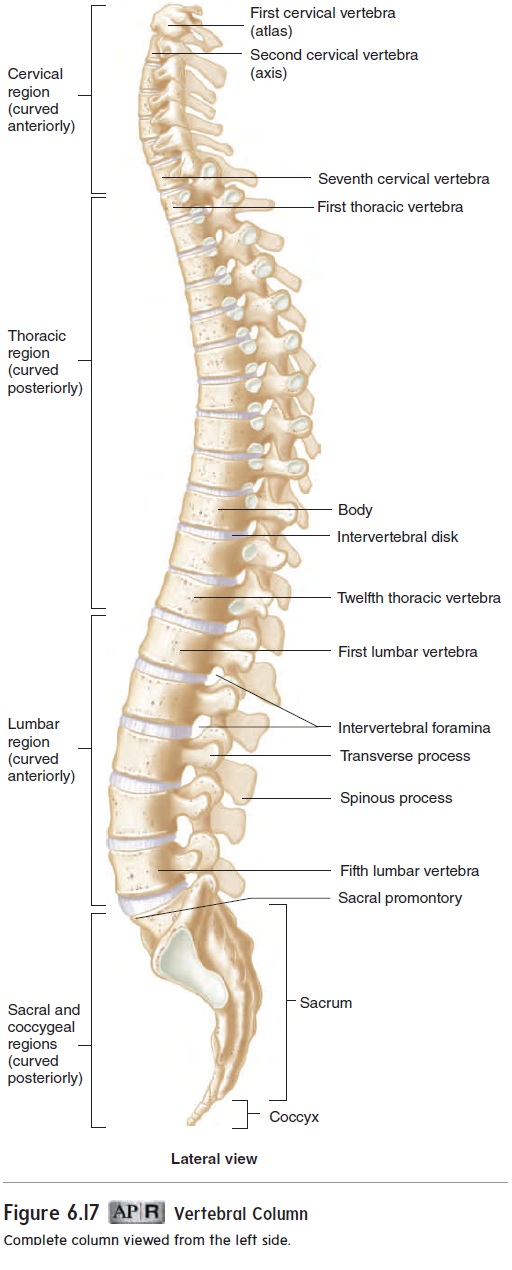
The adult vertebral column has four major curvatures. The cervical region curves anteriorly, the thoracic region curves pos-teriorly, the lumbar region curves anteriorly, and the sacral and coccygeal regions together curve posteriorly.
Abnormal vertebral curvatures are not uncommon. Kyphosis (kı̄ -fō ′ sis) is an abnormal posterior curvature of the spine, mostly in the upper thoracic region, resulting in a hunchback condition. Lordosis(lōr-dō′sis; curving forward) is an abnormal anterior curvature of the spine, mainly in the lumbar region, resulting in a swayback condition. Scoliosis (skō-lē-ō′\sis) is an abnormal lateral curvature of the spine.
The vertebral column performs the following five major func-tions: (1) supports the weight of the head and trunk; (2) protects the spinal cord; (3) allows spinal nerves to exit the spinal cord;(4) provides a site for muscle attachment; and (5) permits move-ment of the head and trunk.
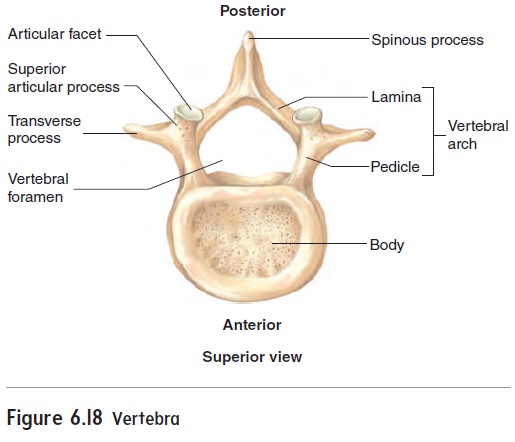
General Plan of the Vertebrae
Each vertebra consists of a body, an arch, and various processes (figure 6.18). The weight-bearing portion of each vertebra is the body. The vertebral bodies are separated by intervertebraldisks (see figure 6.17), which are formed by fibrocartilage. The vertebral arch surrounds a large opening called the vertebral foramen. The vertebral foramina of all the vertebrae form the ver-tebral canal, where the spinal cord is located. The vertebral canalprotects the spinal cord from injury. Each vertebral arch consists of two pedicles (ped′\ı̆-klz), which extend from the body to the transverse process of each vertebra, and twolaminae (lam′\i-nē; thin plates), which extend from the transverse processes to the spinous process. A transverse process extends laterally from each side of the arch, between the pedicle and lamina, and a single spi-nous process projects dorsally from where the two laminae meet.The spinous processes can be seen and felt as a series of lumps down the midline of the back (see figure 6.24b). The transverse and spinous processes provide attachment sites for the muscles that move the vertebral column. Spinal nerves exit the spinal cord through the intervertebral foramina, which are formed by notch-es in the pedicles of adjacent vertebrae (see figure 6.17). Each vertebra has a superior and an inferior articular process where the vertebrae articulate with each other. Each articular process has a smooth “little face” called an articular facet (fas′et).
Regional Differences in Vertebrae
The cervical vertebrae (figure 6.19a–c) have very small bodies, except for the atlas, which has no body. Because the cervical vertebrae\ are relatively delicate and have small bodies, dislocations and fractures are more common in this area than in other regions of the vertebral column. Each of the transverse processes has a transverse foramen through which the vertebral arteries pass toward the brain. Several of the cervical vertebrae also have partly split spinous processes. The first cervical vertebra (figure 6.19a) is called the atlas because it holds up the head, as Atlas in classical mythology held up the world. Movement between the atlas and the occipital bone is responsible for a “yes” motion of the head. It also allows a slight tilting of the head from side to side. The second

cervical vertebra (figure 6.19b) is called the axis because a consid-erable amount of rotation occurs at this vertebra, as in shaking the head “no.” This rotation occurs around a process called the dens (denz), which protrudes superiorly from the axis.
The thoracic vertebrae (figure 6.19d) possess long, thin spinous processes that are directed inferiorly. The thoracic vertebrae also have extra articular facets on their lateral surfaces that articulatewith the ribs.
The lumbar vertebrae (figure 6.19e) have large, thick bodiesand heavy, rectangular transverse and spinous processes. Because the lumbar vertebrae have massive bodies and carry a large amount of weight, ruptured intervertebral disks are more com-mon in this area than in other regions of the column. The superiorarticular facets of the lumbar vertebrae face medially, whereas the inferior articular facets face laterally. This arrangement tends to “lock” adjacent lumbar vertebrae together, giving the lumbar part of the vertebral column more strength. The articular facets in other regions of the vertebral column have a more “open” position, allowing for more rotational movement but less stability than in the lumbar region.
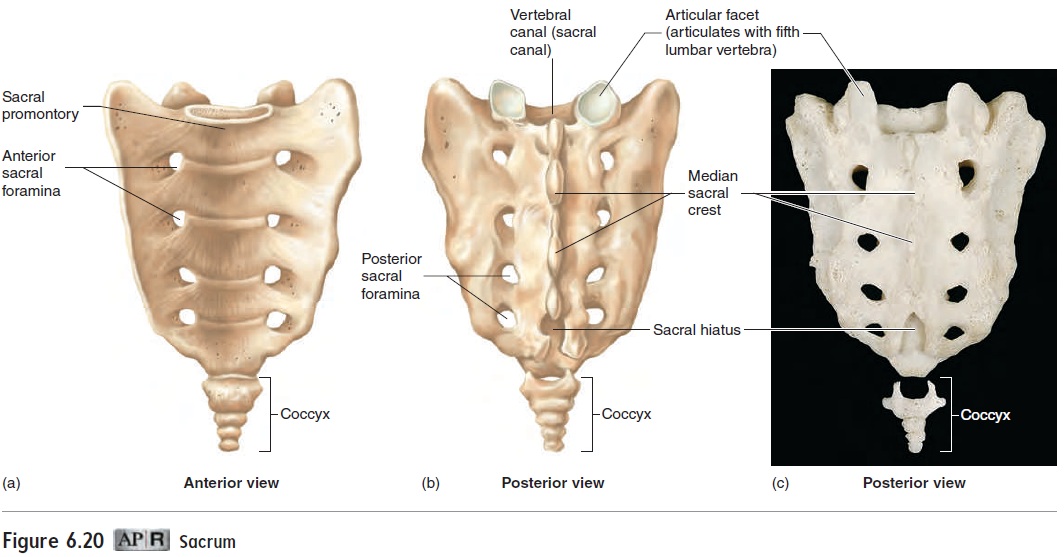
The five sacral vertebrae are fused into a single bone called the sacrum (figure 6.20). The spinous processes of the first four sacral vertebrae form the median sacral crest. The spinous pro-cess of the fifth vertebra does not form, leaving a sacral hiatus (hı̄-ā-tŭs) at the inferior end of the sacrum, which is often the site of “caudal” anesthetic injections given just before childbirth. The anterior edge of the body of the first sacral vertebra bulges to form the sacral promontory (prom′\on-tō-rē) (see figure 6.17), a landmark that can be felt during a vaginal examination. It is used as a reference point to determine if the pelvic openings are large enough to allow for normal vaginal delivery of a baby.
The coccyx, or tailbone, usually consists of four more-or-less fused vertebrae. The vertebrae of the coccyx do not have the typical structure of most other vertebrae. They consist of extremely reduced vertebral bodies, without the foramina or processes, usu-ally fused into a single bone. The coccyx is easily broken when a person falls by sitting down hard on a solid surface or in women during childbirth.
Rib Cage
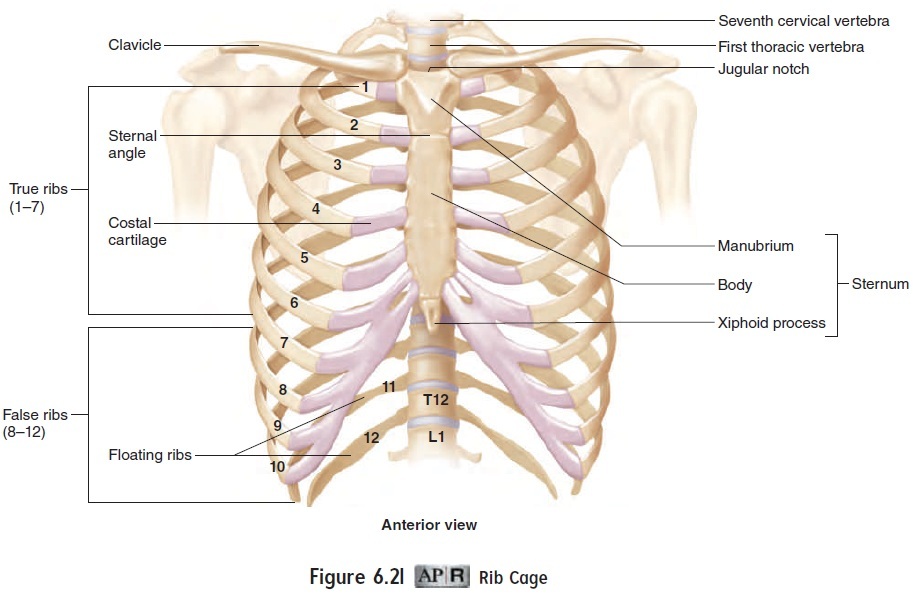
The rib cage protects the vital organs within the thorax and pre-vents the collapse of the thorax during respiration. It consists of the thoracic vertebrae, the ribs with their associated cartilages, and the sternum (figure 6.21).
Ribs and Costal Cartilages
The 12 pairs of ribs can be divided into true ribs and false ribs. The true ribs, ribs 1–7, attach directly to the sternum by means of costalcartilages. The false ribs, ribs 8–12, do not attach directly to the ster-num. Ribs 8–10 attach to the sternum by a common cartilage; ribs 11 and 12 do not attach at all to the sternum and are called floating ribs.
Sternum
The sternum (ster′\nŭm), or breastbone (figure 6.21), is divided into three parts: the manubrium (mă-nū′\brē-ŭm; handle), the body, and the xiphoid (zif′\oyd, zı̄ ′\foyd; sword) process. The sternum resem-bles a sword, with the manubrium forming the handle, the body forming the blade, and the xiphoid process forming the tip.
At the superior end of the sternum, a depression called the jugular notch is located between the ends of the clavicles where they articulate with the sternum. A slight elevation, called the sternal angle, can be felt at the junction of the manubrium and the body of the sternum. This junction is an important landmark because it identifies the location of the second rib. This identification allows the ribs to be counted; for example, it can help a health professional locate the apex of the heart, which is between the fifth and sixth ribs.
The xiphoid process is another important landmark of the sternum. During cardiopulmonary resuscitation (CPR), it is very important to place the hands over the body of the sternum rather than over the xiphoid process. Pressure applied to the xiphoid process can drive it into an underlying abdominal organ, such as the liver, causing internal bleeding.
Related Topics