Chapter: Medicine and surgery: Cardiovascular system
Atrial septal defects - congenital heart disease
Atrial septal defects
Definition
Pathological flow of blood between the atria through a septal defect.
Incidence
10% of congenital heart defects.
Sex
F > M
Aetiology
Defects in the ostium primum occur in patients with Down syndrome often as part of an atrioventricular septal defect.
Pathophysiology
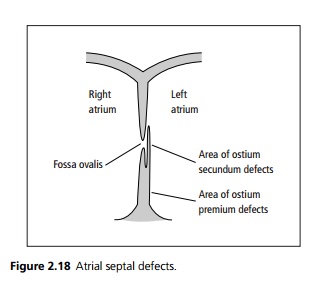
The atrial septum is embryologically made up of two parts: the ostium primum and the ostium secundum, which forms a flap over the defect in the ostium primum (see Fig. 2.18). In the foetal circulation right heart pressures are higher than left due to the extensive vasoconstriction within the lungs. This allows blood to flow through the fossa ovalis and hence shunts blood away from the non-functioning lungs. In normal individuals at birth the vasculature within the lungs dilate at birth and hence the right heart pressures fall. Once the left atrial pressure exceeds the right, the ostium secundum flap closes the fossa ovalis.
· Ostium secundum defects (70%) rarely produce symptoms before middle age.
· Ostium primum defects (30%) are situated lower in the septum and are often associated with abnormalities of the atrioventricular valves.
The shunting of blood from left to right increases the volume of blood passing through the right side of the heart leading to right ventricular volume overload and may eventually lead to right heart failure. Prolonged high volume blood flow through lungs can occasionally lead to pulmonary hypertension due to changes in the pulmonary vasculature similar to ventricular septal defects.
Clinical features
Atrial septal defects are often asymptomatic in childhood but may cause right heart failure and arrhythmias (especially atrial fibrillation) in later life. On examination there is a fixed widely split second heart sound due to the high volumes flowing through the right side of the heart and the equalisation of right and left pressures during respiration.
Flow through the ASD does not cause a murmur, a systolic murmur is usually heard due to increased flow through the pulmonary valve. A diastolic murmur may also occur due to flow across the tricuspid valve.
Rarely patients may present with paradoxical emboli (where thrombus from a deep vein thrombosis crosses the atrial septal defect and causes stroke or peripheral arterial occlusion).
Investigations
· Chest X-ray may show prominent pulmonary arteries and cardiomegaly.
· ECG often shows some degree of right bundle branch block. Ostium secundum tends to produce right axis deviation, whereas ostium primum produces left axis deviation.
· Echocardiogram demonstrates abnormal septal motion and can show blood flow between the atria.
Management
In ostium secundum defect repair is safe and advisable. The defect may be closed using an umbrella-shaped occluder placed at cardiac catheterisation. Traditional open surgical repair requires cardiopulmonary bypass and may use a pericardial or Dacron patch to close the defect. Surgical intervention in ostium primum defects is more complex due to involvement of the atrioventricular valves.
Related Topics