Chapter: Essentials of Psychiatry: Eating Disorders
Anorexia Nervosa
Anorexia
Nervosa
Definition
The
DSM-IV-TR criteria require the individual to be significantly underweight for
age and height. Although it is not possible to set a single weight loss
standard that applies equally to all individu-als, DSM-IV-TR provides a
benchmark of 85% of the weight con-sidered normal for age and height as a
guideline. Despite being of an abnormally low body weight, individuals with
anorexia ner-vosa are intensely afraid of gaining weight and becoming fat, and
remarkably, this fear typically intensifies as the weight falls.
DSM-IV-TR
criterion C requires a disturbance in the per-son’s judgment about his or her
weight or shape. For example, despite being underweight, individuals with
anorexia nervosa often view themselves or a part of their body as being too
heavy. Typically, they deny the grave medical risks engendered by their
semistarvation and place enormous psychological importance on whether they have
gained or lost weight. For example, some-one with anorexia nervosa may feel
intensely distressed if her or his weight increases by half a pound. Finally,
criterion D requires that women with anorexia nervosa be amenorrheic.
The
DSM-IV-TR criteria for anorexia nervosa are gener-ally consistent with recent
definitions and descriptions of this ill-ness. In addition, in DSM-IV-TR, a new
subtyping scheme was introduced. DSM-IV-TR suggests that individuals with
anorexia nervosa be classed as having one of two variants, either the
binge-eating/purging type or the restricting type. Individuals with the
re-stricting type of anorexia nervosa do not engage regularly in either
binge-eating or purging and, compared with individuals with the binge-eating/purging
form of the disorder, are not as likely to abuse alcohol and other drugs,
exhibit less mood lability and are less ac-tive sexually. There are also
indications that the two subtypes may differ in their response to
pharmacological intervention.
Epidemiology
Anorexia nervosa is a relatively rare illness. Even among high-risk groups, such as adolescent girls and young women, the preva-lence of strictly defined anorexia nervosa is only about 0.5%. The prevalence rates of partial syndromes are substantially higher. Despite the infrequent occurrence of anorexia nervosa, most studies suggest that its incidence has increased significantly dur-ing the last 50 years, a phenomenon usually attributed to changes in cultural norms regarding desirable body shape and weight Anorexia nervosa usually affects women; the ratio of men to women is approximately 1 : 10 to 1 : 20. Anorexia nervosa oc-curs primarily in industrialized and affluent countries and some data suggest that even within those countries, anorexia nervosa is more common among the higher socioeconomic classes. Some occupations, such as ballet dancing and fashion modeling, appear to confer a particularly high risk for the development of anorexia nervosa. Thus, anorexia nervosa appears more likely to develop in an environment in which food is readily available but in which, for women, being thin is somehow equated with higher or special achievement.
Etiology
At
present, the etiology of anorexia nervosa is fundamentally unknown. However,
from several sources, such as the epidemio-logical data just reviewed, it is
possible to identify risk factors whose presence increases the likelihood of
anorexia nervosa. It is also possible to describe the course and complications
of the syndrome and to suggest interactions between features of the dis-order,
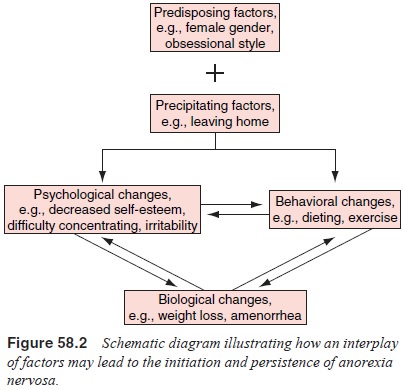
for example, between malnutrition and psychiatric illness. Thus, as indicated
in Figure 58.2, the difficulties that lead to the development of anorexia
nervosa may be distinct from the forces that intensify the symptoms and
perpetuate the illness once it has begun.
Genetic and Twin Studies
Anorexia nervosa occurs more frequently in biological relatives of patients who present with the disorder. The prevalence rate of anorexia nervosa among sisters of patients is estimated to be approximately 6%; the morbid risk among other relatives ranges from 2 to 4%. Some evidence for a genetic component in the etiol-ogy of anorexia nervosa comes from twin studies, which reported substantially higher concordance rates for monozygotic than for dizygotic twin pairs (Klump et al., 2001). However, conclusive data for genetic transmission of the disorder are not yet available
Family Studies
Individual
psychiatric disorders in parents, dysfunctional fam-ily relationships and
impaired family interaction patterns have been implicated in the etiology of
anorexia nervosa. Mothers of individuals with anorexia nervosa are often
described as over-protective, intrusive, perfectionistic and fearful of
separation; fathers are described as withdrawn, passive, emotionally
con-stricted, obsessional, moody and ineffectual. Family systems theorists have
suggested that impaired family interactions such as pathological enmeshment,
rigidity, overprotectiveness, and difficulties confronting and resolving
conflicts are central fea-tures of anorexic pathology. However, few empirical
studies have been conducted to date, particularly studies that also examine
psychiatrically or medically ill comparison groups. Therefore, the precise role
of the family in the development and course of anorexia nervosa, although
undoubtedly important, has not been clearly delineated.
Psychosocial Factors
The
increased prevalence of anorexia nervosa has been connected to the current
emphasis in contemporary Western society on an unrealistically thin appearance
in women. There is substantial evidence that a desire to be slim is common
among middle- and upper-class white women and that this emphasis on slimness
has increased significantly during the past several decades. In the USA,
anorexia nervosa develops much more frequently in white adolescents than in
adolescents from other racial groups. It has been suggested that a variety of
characteristics may protect African-American girls from having eating
disorders, including more acceptance of being overweight, more satisfaction
with their body image and less social pressure regarding weight.
It has
also been suggested that the emphasis of contem-porary Western society on
achievement and performance in women, which is a shift from the more
traditional emphasis on deference, compliance and unassertiveness, has left
many young women vulnerable to the development of eating disorders such as
anorexia nervosa. These multiple and contradictory role demands are embodied
within the modern concept of a superwoman who performs all of the expected
roles (e.g., is competent, ambitious and achieving, yet also feminine,
nurturing and sexual) and, in addition, devotes considerable attention to her appearance
(Gordon, 1990).
Psychodynamic Factors
Various
psychoanalytic theories have been postulated (e.g., de-fense against fantasies
of oral impregnation; underlying deficits in the development of object
relations; deficits in self-structure), but such hypotheses are difficult to
verify. Bruch (1973, 1982) suggested that anorexia nervosa stems from failures
in early at-tachment, attempts to cope with underlying feelings of
ineffec-tiveness and inadequacy, and an inability to meet the demands of adolescence
and young adulthood. These ideas, as well as her conceptualization that the
single-minded focus on losing weight in anorexia nervosa is the concrete
manifestation of a struggle to achieve a sense of identity, purpose,
specialness and control, are compelling and clinically useful.
Cognitive–behavioral theo-ries emphasize the distortions and dysfunctional
thoughts (e.g., dichotomous thinking) that may stem from various causal
fac-tors, all of which eventually focus on the belief that it is essential to be
thin.
Although
the existence of a specific predisposing person-ality style has not been
conclusively documented, certain traits have commonly been reported among women
with anorexia nervosa. Women hospitalized for anorexia nervosa have greater
self-discipline, conscientiousness and emotional caution than women
hospitalized for bulimia nervosa and women with no eat-ing disorders. In
addition, even after they have recovered from their illness, women who have had
anorexia nervosa tend to avoid risks and to exhibit high levels of caution in
emotional expression and strong compliance with rules and moral standards.
Developmental Factors
Because
anorexia nervosa typically begins during adolescence, developmental issues are
thought to play an important etiologi-cal role. Critical challenges at this
time of life include the need to establish independence, a well-defined
personal identity, ful-filling relationships, and clear values and principles
to govern one’s life. Family struggles, conflicts regarding sexuality and
pressures regarding increased heterosexual contact are also com-mon. However,
it is not clear that difficulties over these issues are more salient for
individuals who will develop anorexia nervosa than for other adolescents.
Depression has been implicated as a nonspecific risk factor, and higher levels
of depressive symptoms as well as insecurity, anxiety and self-consciousness
have been documented in adolescent girls in comparison with adolescent boys.
Similarly, the progression of physical and sexual matura-tion and the
concomitant increase in women’s percentage of body fat may have a substantial
impact on the self-image of adolescent girls, particularly because the
relationship between self-esteem and satisfaction with physical appearance and
body characteris-tics is stronger in women than in men.
Pathophysiology
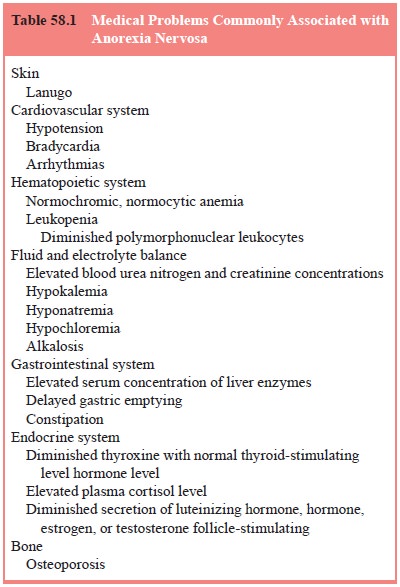
An
impressive array of physical disturbances has been docu-mented in anorexia
nervosa and the physiological bases of many are understood (Table 58.1). Most
of these physical disturbances appear to be secondary consequences of
starvation, and it is not clear whether or how the physiological disturbances
described here contribute to the development and maintenance of the
psy-chological and behavioral abnormalities characteristic of ano-rexia
nervosa. The remainder of this section briefly describes the major physical
abnormalities of anorexia nervosa and what is understood about their etiology.
The
central nervous system is clearly affected. Computed tomography has
demonstrated that individuals with anorexia ner-vosa have enlarged ventricles,
an abnormality that improves with weight gain. The cerebrospinal fluid
concentrations of a variety of neurotransmitters and their metabolites are
altered in under-weight patients with anorexia nervosa and tend to normalize as
weight is restored. An intriguing exception may be the serotonin metabolite
5-hydroxyindoleacetic acid, which has been reported to be elevated in the
cerebrospinal fluid of patients with anorexia nervosa after they have achieved
a normal or near-normal weight. Kaye (1997) has suggested that the elevated
5-hydroxyindoleace-tic acid levels may reflect a serotoninergic abnormality
that is tied to the obsessional traits often observed in anorexia nervosa.
Some of
the most striking physiological alterations in ano-rexia nervosa are those of
the hypothalamic–pituitary–gonadal axis. In women, estrogen secretion from the
ovaries is markedly reduced, accounting for the occurrence of amenorrhea. In
analo-gous fashion, testosterone production is diminished in men with anorexia
nervosa. The decrease in gonadal steroid production is due to a reduction in
the pituitary’s secretion of the gonadotropins luteinizing hormone and
follicle-stimulating hormone, which in turn is secondary to diminished release
of gonadotropin-releasing
hormone
from the hypothalamus. Therefore, the amenorrhea of anorexia nervosa is
properly viewed as a type of hypothalamic amenorrhea. It is of interest that in
a significant minority amenor-rhea begins before substantial weight loss has
occurred, suggest-ing that factors other than malnutrition, such as
psychological distress, contribute significantly to the disruption of the
repro-ductive endocrine system.
In an
adult with anorexia nervosa, the status of the hy-pothalamic–pituitary–gonadal
axis resembles that of a pubertal or prepubertal child – the secretion of
estrogen or testosterone, of luteinizing hormone and follicle-stimulating
hormone and of go-nadotropin-releasing hormone is reduced. This endocrinological
picture may be contrasted with that of postmenopausal women who have a similar
reduction in estrogen secretion but who, un-like women with anorexia nervosa,
show increased pituitary go-nadotropin secretion. Furthermore, even the
circadian patterns of luteinizing hormone and follicle-stimulating hormone
secretion in adult women with anorexia nervosa closely resemble the pat-terns
normally seen in pubertal and prepubertal girls. Although similar abnormalities
are also seen in other forms of hypotha-lamic amenorrhea and are therefore not
specific to anorexia ner-vosa, it is nonetheless striking that this syndrome is
accompanied by a physiological arrest or regression of the reproductive
endo-crine system.
The
functioning of other hormonal systems is also disrupted in anorexia nervosa,
although typically not as profoundly as is the reproductive axis. Presumably as
part of the metabolic response to semistarvation, the activity of the thyroid
gland is reduced Plasma thyroxine levels are somewhat diminished, but the
plasma level of the pituitary hormone and thyroid-stimulating hormone is not
elevated. The activity of the hypothalamic–pituitary–adrenal axis is increased,
as indicated by elevated plasma levels of cortisol and by resistance to
dexamethasone suppression. The regulation of vasopressin (antidiuretic hormone)
secretion from the posterior pituitary is disturbed, contributing to the
development of partial diabetes insipidus in some individuals.
Anorexia
nervosa is often associated with the develop-ment of leukopenia and of a
normochromic, normocytic anemia of mild to moderate severity. Surprisingly,
leukopenia does not appear to result in a high vulnerability to infectious
illnesses. Se-rum levels of liver enzymes are sometimes elevated, particularly
during the early phases of refeeding, but the synthetic function of the liver
is rarely seriously impaired so that the serum albu-min concentration and the
prothrombin time are usually within normal limits. Serum cholesterol levels are
sometimes elevated in anorexia nervosa, although the basis of this abnormality
re-mains obscure. In some patients, self-imposed fluid restriction and
excessive exercise produce dehydration and elevations of se-rum creatinine and
blood urea nitrogen. In others, water loading may lead to hyponatremia. The
status of serum electrolytes is a reflection of the individual’s salt and water
intake and the nature and the severity of the purging behavior. A common
pattern is hypokalemia, hypochloremia and mild alkalosis resulting from frequent
and persistent self-induced vomiting.
It has
become clear that individuals with anorexia ner-vosa have decreased bone
density compared with age- and sex-matched peers and, as a result, are at
increased risk for fractures. Low levels of estrogen, high levels of cortisol
and poor nutrition have been cited as risk factors for the development of
reduced bone density in anorexia nervosa. Theoretically, estrogen treat-ment
might reduce the risk of osteoporosis in women who are chronically amenorrheic
because of anorexia nervosa, but con-trolled studies indicate that this
intervention is of limited, if any, benefit.
Abnormalities
of cardiac function include bradycardia and hypotension, which are rarely
symptomatic. The pump function of the heart is compromised, and congestive
heart failure occa-sionally develops in individuals during overly rapid
refeeding. The electrocardiogram shows sinus bradycardia and a number of
nonspecific abnormalities. Arrhythmias may develop, often in association with
fluid and electrolyte disturbances. It has been suggested that significant
prolongation of the QT interval may be a harbinger of life-threatening
arrhythmias in some individ-uals with anorexia nervosa, but this has not been
conclusively demonstrated.
The
motility of the gastrointestinal tract is diminished, leading to delayed
gastric emptying and contributing to com-plaints of bloating and constipation.
Rare cases of acute gastric dilatation or gastric rupture, which is often
fatal, have been re-ported in individuals with anorexia nervosa who consumed
large amounts of food when binge-eating.
As
already noted, virtually all of the physiological abnor-malities described in
individuals with anorexia nervosa are also seen in other forms of starvation,
and most improve or disappear as weight returns to normal. Therefore, weight
restoration is essen-tial for physiological recovery. More surprisingly,
perhaps, weight restoration is believed to be essential for psychological
recovery as well. Accounts of human starvation amply document the pro-found
impact of starvation on mental health. Starving individuals lose their sense of
humor, their interest in friends and family fadesand mood generally becomes
depressed. They may develop pe-culiar behavior similar to that of patients with
anorexia nervosa, such as hoarding food or concocting bizarre food
combinations. If starvation disrupts psychological and behavioral functioning
in normal individuals, it presumably does so as well in those with anorexia
nervosa. Thus, correction of starvation is a prerequisite for the restoration
of both physical and psychological health.
Diagnosis and Differential Diagnosis
Phenomenology
Anorexia
nervosa often begins innocently. Typically, an adoles-cent girl or young woman
who is of normal weight or, perhaps, a few pounds overweight decides to diet.
This decision may be prompted by an important but not extraordinary life event,
such as leaving home for camp, attending a new school, or a casual unflattering
remark by a friend or family member. Initially, the dieting seems no different
from that pursued by many young women, but as weight falls, the dieting
intensifies. The restric-tions become broader and more rigid; for example,
desserts may first be eliminated, then meat, then any food that is thought to
contain fat. The person becomes increasingly uncomfortable if she is seen
eating and avoids meals with others. Food seems to assume a moral quality so
that vegetables are viewed as “good” and anything with fat is “bad”. The
individual has idiosyncratic rules about how much exercise she must do and
when, where and how she can eat.
Food
avoidance and weight loss are accompanied by a deep and reassuring sense of
accomplishment, and weight gain is viewed as a failure and a sign of weakness.
Physical activity, such as running or aerobic exercise, often increases as the
dieting and weight loss develop. Inactivity and complaints of weakness usually
occur only when emaciation has become extreme. The person becomes more serious
and devotes little effort to anything but work, dieting and exercise. She may
become depressed and emotionally labile, socially withdrawn and secretive and
she may lie about her eating and her weight. Despite the profound distur-bances
in her view of her weight and of her calorie needs, reality testing in other
spheres is intact, and the person may continue to function well in school or at
work. Symptoms usually persist for months or years until, typically at the
insistence of friends or family, the person reluctantly agrees to see a physician.
In
general, anorexia nervosa is not difficult to recognize. Uncertainty
surrounding the diagnosis sometimes occurs in young adolescents, who may not
clearly describe a drive for thin-ness and the fear of becoming fat. Rather,
they may acknowl-edge only a vague concern about consuming certain foods and an
intense desire to exercise. It can also be difficult to elicit the distorted
view of shape and weight (criterion C) from patients who have had anorexia
nervosa for many years. Such individu-als may state that they realize they are
too thin and may make superficial efforts to gain weight, but they do not seem
particu-larly concerned about the physical risks or deeply committed to
increasing their calorie consumption.
Assessment
Special Issues in Psychiatric Examination and History
In
assessing individuals who may have anorexia nervosa, it is important to obtain
a weight history including the individual’s highest and lowest weights and the
weight he or she would like to be now. For women, it is useful to know the
weight at which menstruation last occurred, because it provides an indi-cation
of what weight is normal for that individual. The patient should be asked to
describe a typical day’s food intake and any food restrictions and dietary
practices such as vegetarian-ism. The psychiatrist should ask whether the
patient ever loses control over eating and engages in binge-eating and, if so,
the amounts and types of food eaten during such episodes. The use of
self-induced vomiting, laxatives, diuretics, enemas, diet pills, and syrup of
ipecac to induce vomiting should also be queried.
Probably
the greatest problem in the assessment of pa-tients with anorexia nervosa is
their denial of the illness and their reluctance to participate in an
evaluation. A straightforward but supportive and nonconfrontational style is
probably the most useful approach, but it is likely that the patient will not
acknowl-edge significant difficulties in eating or with weight and will
ra-tionalize unusual eating or exercise habits. It is therefore helpful to
obtain information from other sources such as the patient’s family.
Physical Examination and Laboratory Findings
The
patient should be weighed, or a current weight should be obtained from the
patient’s general physician. Blood pressure, pulse and body temperature are
often below the lower limit of normal. On physical examination, lanugo, a fine,
downy hair nor-mally seen in infants, may be present on the back or the face.
The extremities are frequently cold and have a slight red–purple color
(acrocyanosis). Edema is rarely observed at the initial pres-entation but may
develop transiently during the initial stages of refeeding.
The basis
for laboratory abnormalities is presented in the earlier section on
pathophysiology. Common findings are a mild to moderate normochromic,
normocytic anemia and leukope-nia, with a deficit in polymorphonuclear
leukocytes leading to a relative lymphocytosis. Elevations of blood urea
nitrogen and serum creatinine concentrations may occur because of dehydra-tion,
which can also artificially elevate the hemoglobin and he-matocrit. A variety
of electrolyte abnormalities may be observed, reflecting the state of hydration
and the history of vomiting and diuretic and laxative abuse. Serum levels of liver
enzymes are usually normal but may transiently increase during refeeding.
Cholesterol levels may be elevated.
The
electrocardiogram typically shows sinus bradycardia and, occasionally, low QRS
voltage and a prolonged QT interval; a variety of arrhythmias have also been
described.
Differences in Presentation
The
symptoms of anorexia nervosa are remarkably homogene-ous, and differences
between patients in clinical manifestations are fewer than in most psychiatric
illnesses. As described before, younger patients may not express verbally the
characteristic fear of fatness or the overconcern with shape and weight, and
some patients with longstanding anorexia nervosa may express a desire to gain
weight but be unable to make persistent changes in their behavior. It has been
suggested that in other cultures, the ration-ale given by patients for losing
weight differs from the fear of fatness characteristic of cases in North
America.
Men have
anorexia nervosa far less frequently than women. However, when the syndrome
does develop in a man, it is typical. There may be an increased frequency of
homosexuality among men with anorexia nervosa.
Related Topics