Chapter: Clinical Anesthesiology: Anesthetic Management: Anesthesia for Neurosurgery
Anesthesia for Stereotactic Surgery
Anesthesia for Stereotactic Surgery
Stereotaxis can be employed in treating involuntary movement
disorders, intractable pain, and epilepsy and can also be used when diagnosing
and treating tumors that are located deep within the brain.
These procedures are often performed
under local anesthesia to allow evaluation of the patient. Propofol or
dexmedetomidine infusions are rou-tinely used for sedation and amnesia.
Sedation should be omitted, however, if the patient already has increased ICP.
The ability to rapidly provide con-trolled ventilation and general anesthesia
for emer-gency craniotomy is mandatory, but is complicated by the platform and
localizing frame that is attached to the patient’s head for the procedure.
Although mask ventilation or ventilation through a laryngeal mask airway (LMA)
or orotracheal intubation might be readily accomplished in an emergency, awake
intubation with a fiberoptic bronchoscope prior to positioning and surgery may
be the safest approach when intubation is necessary for a patient whose head is
already in a stereotactic head frame.
Functional neurosurgery is increasingly per-formed for removal
of lesions adjacent to speech and other vital brain centers. Sometimes patients
are managed with an asleep–awake–asleep technique, with or without
instrumentation of the airway. Such operations require the patient to be awake
to par-ticipate in cortical mapping to identify key speech centers, such as
Broca’s area. Patients sleep during the painful periods of surgery (ie, during
opening and closure). LMAs are often employed to assist air-way management
during the asleep portions of these surgeries.
Patients undergo deep brain stimulator
inser-tion for control of movement and other disorders. A stimulator electrode
is placed via a burr hole using radiologic guidance to establish coordinates
for electrode placement. A microelectrode recording (MER) is obtained to
determine the correct place-ment of the stimulator in brain structures. The effect
of stimulation upon the patient is noted. Sedative medications can adversely
affect MER potentials, complicating the location of the correct depth of
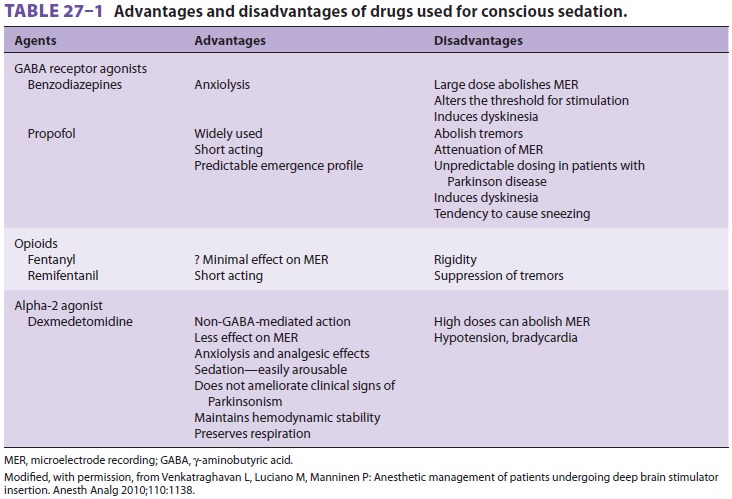
stimulator placement. Dexmedetomidine has been used to provide
sedation to these patients; however, during MER and stimulation testing,
sedative infu-sions should be discontinued to facilitate patient participation
in determining correct electrode placement (Table27–1).
Related Topics